
Axillary lymph node dissection removes a group of lymph nodes from under the arm to check how far breast cancer has spread and to reduce the risk of it progressing further through the lymphatic system. It’s a more extensive procedure than sentinel node biopsy and is reserved for situations where the sentinel node has confirmed cancer or where the extent of nodal disease makes a targeted approach insufficient.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India,
“Axillary dissection is recommended when the nodal burden justifies it the decision is always weighed against the long-term morbidity it carries, because removing nodes that didn’t need removing causes problems that last years.”
Need clarity on whether axillary dissection is part of your breast cancer plan?
What Does Axillary Lymph Node Dissection Involve?
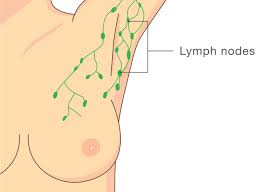
The procedure removes the level one and two axillary nodes sometimes level three as well depending on how extensively disease has spread through the axilla.
- Node Levels Removed: Axillary nodes are grouped into three levels based on their position relative to the pectoralis minor muscle level one and two are removed in most cases while level three is added when disease has clearly moved into the highest axillary group.
- Done Alongside Breast Surgery: Axillary dissection runs in the same operation as lumpectomy or mastectomy rather than as a separate procedure, and breast cancer treatment planning confirms the extent of nodal surgery required before the patient goes to theatre.
- Drain Placement: A surgical drain is placed in the axilla at the end of the procedure to prevent fluid accumulation most patients go home with it in place and return for removal once drainage reduces to an acceptable daily volume.
- Pathology After Surgery: All removed nodes are examined by a pathologist who counts how many contain cancer, which directly affects staging, adjuvant chemotherapy decisions and whether radiation to the axilla is added to the post-operative treatment plan.
The number of nodes removed and how many are positive both feed into decisions that shape everything the oncology team recommends after surgery.
When Is Axillary Dissection Recommended Over Sentinel Biopsy?
Sentinel node biopsy has replaced axillary dissection for most early-stage patients but specific clinical situations still make the more extensive procedure necessary.
- Positive Sentinel Node: When the sentinel node biopsy confirms cancer and the extent of involvement or number of positive nodes meets criteria for full dissection, the surgical team proceeds to clearing the axilla rather than relying on radiation alone to manage it.
- Clinically Positive Nodes: Nodes that are palpable, firm or confirmed positive on pre-operative imaging or biopsy indicate disease beyond the sentinel node operating on those nodes directly rather than sampling the first draining node is what the clinical picture requires.
- After Failed Sentinel Mapping: Occasionally the tracer fails to identify a sentinel node clearly this happens in patients who have had prior axillary surgery or radiation and dissection becomes the only reliable way to assess nodal status surgically.
- Recurrent Axillary Disease: When breast cancer recurs in the axillary nodes after previous sentinel biopsy, robotic cancer surgery or conventional dissection clears the affected nodal tissue and restages the disease for the next phase of treatment.
The morbidity of axillary dissection particularly lymphoedema means the decision is always carefully weighed, and for more on minimally invasive approaches to cancer surgery, our blog on minimally invasive cancer surgery covers this in detail.
Why Choose Dr. Sandeep Nayak for Breast Cancer Treatment ?
Dr. Sandeep Nayak brings 24 years of surgical oncology experience, DNB qualifications in Surgical Oncology and General Surgery and a fellowship in Laparoscopic and Robotic Onco-Surgery to every axillary surgery decision in breast cancer including sentinel biopsy and full dissection. He heads Oncology Services across Karnataka and leads breast cancer surgery at KIMS Hospital, Bangalore, with originator credits for RABIT and over 25 published clinical studies. Patients who want clarity on whether dissection is genuinely needed for their case are seen here with every decision going through tumour board review. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
What is the difference between sentinel node biopsy and axillary dissection?
Sentinel biopsy removes one to three nodes for assessment while axillary dissection removes the entire group of nodes from under the arm.
How many lymph nodes are removed in axillary dissection?
Typically ten to thirty nodes depending on the level of dissection performed and individual anatomy of the axilla.
What is the main risk of axillary lymph node dissection?
Lymphoedema chronic arm swelling from disrupted lymphatic drainage is the most significant long-term risk of axillary dissection.
How long does recovery from axillary dissection take?
Most patients manage normal daily activities within two to three weeks though physiotherapy for shoulder movement continues for several weeks after that.
References
-
- National Cancer Institute — Breast Cancer Surgery
- National Institutes of Health — Axillary Lymph Node Management
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.
