
Breast reconstruction after mastectomy uses either implant-based reconstruction with silicone or saline devices placed under the chest muscle, or autologous flap reconstruction using the patient’s own tissue from the abdomen, back or thighs. Implants offer shorter surgery, faster recovery and no donor site scarring but feel firmer and may need replacing over time. Flap techniques create natural-feeling breasts that age with the body and handle post-mastectomy radiation far better than any implant can.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India,
“Reconstruction is part of the surgical plan from the start, not an afterthought. Getting the right method for that specific patient depends on the oncological plan and the patient’s body together.”
Facing mastectomy and trying to decide between implant and flap reconstruction?
What Is Implant Reconstruction and Who Is It For?
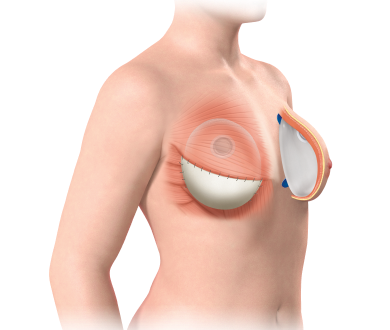
Implant reconstruction is the faster, less complex option and works well in the right clinical situation.
- How It Works: A silicone or saline implant is placed under the chest muscle either immediately at mastectomy or staged using a tissue expander first that gradually stretches the skin before the final implant is inserted weeks later.
- Shorter Recovery: No donor site means faster overall recovery than flap procedures and most patients are discharged sooner and return to daily activity more quickly than those having tissue transferred from elsewhere on the body.
- Radiation Makes It Unsuitable: Post-mastectomy radiation significantly increases implant complication rates including capsular contracture and device failure and breast cancer treatment centres typically recommend flap reconstruction for patients who need chest wall radiation after mastectomy.
- Long-Term Considerations: Implants may need replacement over time and don’t age the same way natural tissue does while flap reconstruction using the patient’s own tissue behaves more naturally as the body changes with age and weight over years.
Implant reconstruction is the most common first choice where radiation isn’t anticipated and the patient’s anatomy supports it without requiring complex donor site surgery.
Implant vs Flap: How the Two Approaches Compare
|
Implant Reconstruction |
Flap Reconstruction |
|
|---|---|---|
|
Material |
Silicone or saline device |
Patient’s own tissue from back or abdomen |
|
Recovery Time |
Faster, shorter hospital stay |
Longer, donor site also heals |
|
Natural Feel |
Firmer, less natural |
More natural, ages with body |
|
After Radiation |
Not recommended |
Better choice when radiation follows |
|
Replacement Needed |
Possibly over time |
Generally permanent |
|
Operative Duration |
Shorter |
Four to eight hours |
- Flap Reconstruction Handles Radiation Better: Tissue transferred from the patient’s own body tolerates radiation far better than a synthetic implant and for Stage 3 patients needing post-mastectomy chest wall radiation, flap options produce significantly more predictable long-term results.
- DIEP and TRAM Flaps Use Abdominal Tissue: These procedures harvest tissue from the lower abdomen creating a natural-feeling breast while simultaneously flattening the donor area, which some patients find a welcome additional outcome alongside the reconstruction itself.
- Latissimus Flap Uses Back Tissue: Tissue from the back combined with a small implant underneath is used when abdominal tissue isn’t suitable and robotic cancer surgery centres increasingly perform these with minimally invasive donor site techniques to reduce back scarring and recovery time.
- Staged vs Immediate Timing: Both approaches can be done immediately at mastectomy or delayed until after chemotherapy and radiation are complete with timing planned around the oncological treatment sequence rather than reconstruction preference alone.
Reconstruction type and timing are decided together with the surgical oncology team before mastectomy happens and for more on the latissimus flap technique specifically, our blog on latissimus dorsi covers this in detail.
Why Choose Dr. Sandeep Nayak for Breast Cancer Treatment?
Dr. Sandeep Nayak brings 24 years of surgical oncology experience, DNB qualifications in Surgical Oncology and General Surgery and a fellowship in Laparoscopic and Robotic Onco-Surgery to every mastectomy including full reconstruction planning from the start of the surgical discussion. He heads Oncology Services across Karnataka and leads breast cancer surgery at KIMS Hospital, Bangalore, with originator credits for RABIT and over 25 published clinical studies. Patients who want reconstruction discussed as part of their mastectomy plan rather than separately are seen here with every decision going through tumour board review. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
Which reconstruction type feels more natural long term?
Flap reconstruction using the patient’s own tissue generally feels more natural and responds to body changes more predictably than an implant over time.
Can reconstruction be done at the same time as mastectomy?
Both implant and flap reconstruction can be performed immediately at mastectomy or delayed depending on whether radiation follows and patient fitness.
Why is implant reconstruction not recommended after radiation?
Radiation damages chest wall tissue making implant complications including capsular contracture and device failure significantly more likely in irradiated skin.
How long does flap reconstruction surgery take compared to implant?
Flap reconstruction typically runs four to eight hours while implant placement adds one to two hours to the mastectomy operative time.
Reference Links-
- National Cancer Institute — Breast Reconstruction After Mastectomy
- World Health Organization — Breast Cancer Treatment
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.
