What Is HIPEC Treatment for Stage 4 Cancer?
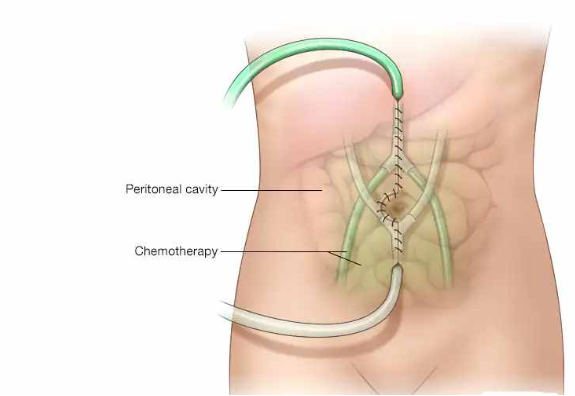
HIPEC treatment for stage 4 cancer is a procedure where a surgeon removes every visible tumour deposit from the abdominal cavity first and then floods the whole cavity with heated chemotherapy for around 90 minutes while the patient is still on the table, and the reason heat matters is that it makes the chemotherapy penetrate tissue more deeply than it would at normal body temperature while keeping the drug concentrated exactly where the cancer is rather than sending it through the whole body the way systemic chemo does.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India, “HIPEC gives selected stage 4 cancer patients a genuine chance at long term survival that systemic chemotherapy alone simply cannot offer them.”
How Does HIPEC Actually Work?
These are the key things that happen during HIPEC treatment:
- Cytoreductive surgery comes first: Every visible tumour deposit on the peritoneum, organs and abdominal surfaces gets removed surgically before the chemotherapy even enters the picture and how completely this is done directly determines how well HIPEC works afterward.
- Heated chemo floods the cavity: Once the surgical removal is complete the abdominal cavity gets filled with chemotherapy heated to around 41 to 43 degrees Celsius and circulated for 60 to 90 minutes reaching surfaces and crevices no systemic chemo ever gets to.
- Heat does two jobs: It makes the chemotherapy penetrate deeper into remaining microscopic cancer cells than it would at normal temperature and it directly damages cancer cells itself because tumour tissue is more sensitive to heat than healthy tissue.
- Systemic exposure stays low: Because the chemo stays inside the abdominal cavity during HIPEC the rest of the body doesn’t absorb the same hit it would from intravenous chemotherapy and that changes what side effects the patient actually experiences.
HIPEC is not a last resort procedure handed to patients when nothing else is left, it’s a carefully selected treatment for patients whose cancer has spread to the peritoneum but nowhere else and who are fit enough to handle a major combined procedure. HIPEC treatment at a specialist surgical oncology centre with the infrastructure and volume to do it properly is a genuinely different conversation from a centre attempting it occasionally.
Who Is HIPEC Suitable for in Stage 4 Cancer?
These are the factors that determine whether HIPEC is realistically on the table for a stage 4 patient:
- Peritoneal spread only: HIPEC works when cancer has spread to the peritoneum but hasn’t moved to the liver, lungs or distant organs because if it has the procedure addresses one area while disease progresses somewhere else entirely.
- Completeness of surgery possible: The peritoneal cancer index score tells the surgeon how widely the tumour has spread inside the abdomen and patients with lower scores where complete removal is achievable get meaningfully better outcomes than those where too much has to be left behind.
- Fit enough for a major procedure: Cytoreductive surgery plus HIPEC is a long complex operation with a real recovery demand and patients need to have the physical reserves to handle it safely because the combination is significantly more intense than either procedure alone.
- Right primary cancer type: Colorectal cancer, appendix cancer, ovarian cancer and mesothelioma spreading to the peritoneum are the cancers where HIPEC has the strongest evidence behind it and where specialist centres are most likely to consider it seriously.
Whether HIPEC is the right call for your specific stage 4 cancer needs detailed staging, a peritoneal cancer index assessment and a surgical oncologist who actually does this regularly enough to know where the limits of the procedure genuinely sit. Ovarian cancer treatment is one of the primary indications for HIPEC at specialist centres in India where peritoneal spread is part of the surgical planning from the start.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
HIPEC is one of the more demanding procedures in surgical oncology and the outcomes are directly tied to how experienced the team doing it actually is. Dr. Sandeep Nayak has been performing cytoreductive surgery and HIPEC for years at a centre built around doing it properly rather than occasionally. He chairs Oncology Services across Karnataka and sees patients at MACS Clinic in Bangalore. Dr. Nayak will look at your staging, your peritoneal cancer index and your overall fitness and tell you honestly whether HIPEC is realistically the right path for your case or whether something else fits better.
Frequently Asked Questions
What is HIPEC treatment for stage 4 cancer?
HIPEC removes all visible tumour from the abdominal cavity surgically then floods it with heated chemotherapy to target remaining microscopic cancer cells directly.
Who is suitable for HIPEC treatment?
Patients with peritoneal spread from colorectal, appendix, ovarian or similar cancers where complete surgical removal is achievable and disease hasn’t spread beyond the abdomen.
Is HIPEC a cure for stage 4 cancer?
For selected patients with peritoneal-only spread HIPEC offers genuine long term survival and in some cases disease-free survival that systemic chemo alone cannot achieve.
What is recovery like after HIPEC?
HIPEC involves a major combined operation and recovery typically takes four to eight weeks in hospital and rehabilitation before returning to normal activity.
Reference links:
- National Cancer Institute. Hyperthermia to Treat Cancer. https://www.cancer.gov/about-cancer/treatment/types/surgery/hyperthermia-fact-sheet
2. American Cancer Society. Chemotherapy. https://www.cancer.org/cancer/managing-cancer/treatment-types/chemotherapy.html
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.