Why Is Gallbladder Cancer Caught Late?
Gallbladder cancer is caught late mostly because it hides in plain sight. Its early symptoms look exactly like gallstones, which are far more common, so the cancer gets overlooked. The gallbladder also sits tucked under the liver, out of easy reach. Often the cancer is only found by chance, during surgery for something else.
According to Dr. Sandeep Nayak, Surgical Oncologist in India, “Gallbladder cancer is one of the most quietly deceptive cancers. The early signs, vague upper abdominal pain, nausea, are identical to ordinary gallstone trouble. So it’s treated as that. By the time clearer signs appear, the disease has usually advanced. A surprising number of cases are only picked up when a gallbladder removed for stones turns out to contain cancer.”
Have ongoing gallbladder symptoms that won’t settle?
Why Does It Stay Hidden So Long?
Several things conspire to keep this cancer out of sight until it’s advanced.
- Gallstone disguise : Early symptoms copy gallstones almost exactly. Pain and nausea get blamed on stones, and the cancer slips through.
- Hidden location : The gallbladder sits under the liver, hard to feel and easy to miss on a quick scan. Small tumours stay invisible.
- No early signs : In its earliest stage the cancer often causes nothing at all. By the time it speaks up, it’s already grown.
- No screening : There’s no routine test for gallbladder cancer like there is for some others. Nobody goes looking until symptoms force it.
This is why imaging matters so much, and the right gallbladder cancer assessment depends on not dismissing persistent symptoms as simple stones.
How Is It Often Discovered?
When gallbladder cancer is found, it’s frequently through routes nobody planned.
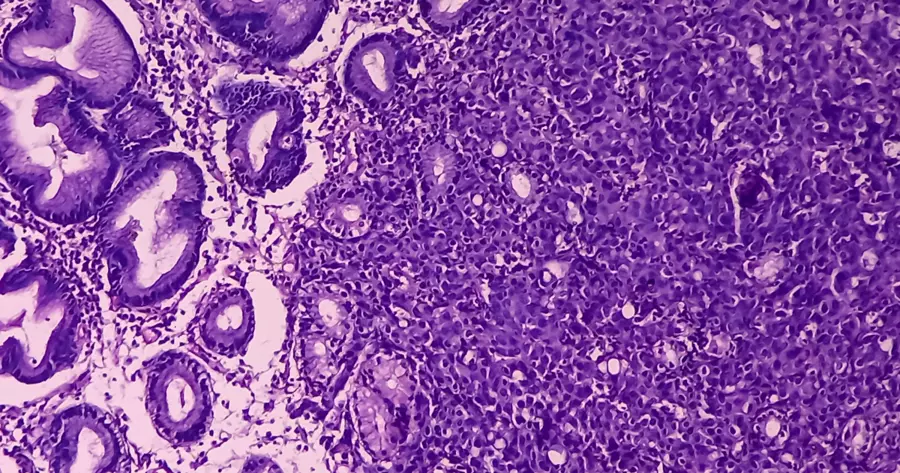
- Incidental finding : A common route. The gallbladder is removed for stones, and the lab report comes back with cancer nobody expected.
- Late symptoms : Jaundice, a hard lump, real weight loss. These bring people in, but they tend to signal advanced disease.
- Imaging by chance : Sometimes a scan done for an unrelated complaint spots a thickened gallbladder wall or a mass. A lucky catch.
- Risk based vigilance : People with long standing gallstones or a calcified gallbladder warrant closer watching. That’s where earlier catches happen.
Recognising which cancer testing applies when symptoms persist is what occasionally turns a late diagnosis into an earlier one.
Why Choose Dr. Sandeep Nayak for Gallbladder Cancer Care?
Dr. Sandeep Nayak is a surgical oncologist with 24 years behind him and a fellowship in laparoscopic and robotic onco-surgery. He treats hepatobiliary cancers, including gallbladder and bile duct disease, where recognising the deceptive early picture makes all the difference. The approach starts with taking persistent gallbladder symptoms seriously rather than assuming stones. That scrutiny is what catches the occasional cancer hiding among them.
Incidental gallbladder cancer needs particular expertise. When cancer turns up unexpectedly in a removed gallbladder, what happens next, proper staging and often a second, more extensive operation, decides the outcome. Handled by an experienced hepatobiliary surgeon, even a late or unexpected diagnosis can still be managed with a clear, structured plan.
Frequently Asked Questions
Why is gallbladder cancer found so late?
Early symptoms mimic gallstones and the gallbladder sits hidden, so cancer goes unnoticed.
Can gallbladder cancer be found by accident?
Yes. Many cases are found incidentally after gallbladder removal for suspected gallstones.
Do gallstones raise gallbladder cancer risk?
Yes. Long standing gallstones and chronic inflammation are major risk factors for it.
What are late symptoms of gallbladder cancer?
Jaundice, persistent right upper abdominal pain, weight loss and a palpable mass.
References
- Gallbladder carcinoma diagnostic challenge — National Library of Medicine
- Incidental gallbladder carcinoma after cholecystectomy — National Library of Medicine
Disclaimer: This blog is for informational and educational purposes only and is not a substitute for professional medical advice or diagnosis.