ISR surgery for rectal cancer in Bangalore is performed by Prof. Dr. Sandeep Nayak at MACS Clinic in Jayanagar and if you’re researching inter-sphincteric resection specifically you’ve probably already been told somewhere that a permanent stoma is your only option and you’re looking for a second opinion that might tell you something different, which is exactly the kind of conversation Dr. Nayak has regularly and honestly with patients who arrive at MACS Clinic having been sent somewhere else first.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “ISR is a technically demanding procedure that gives low rectal cancer patients a realistic chance of avoiding a permanent stoma but it only delivers on that promise when it’s done by a surgeon who has performed it enough times to know its limits and when to use it and when not to.”
Where Can You Get ISR Surgery for Rectal Cancer in Bangalore?
These are the key things to understand about getting ISR surgery in Bangalore at genuine volume:
MACS Clinic Jayanagar: Dr. Sandeep Nayak performs inter-sphincteric resection at MACS Clinic Bangalore as part of a low rectal cancer surgical programme built around sphincter preservation at real volume rather than ISR offered occasionally when a suitable case arrives and the surgeon decides to attempt it.
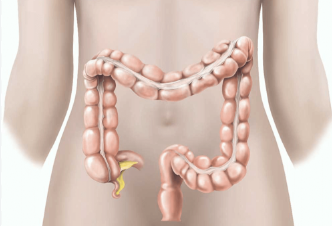
Volume question to ask: ISR dissects the inter-sphincteric plane between the internal and external anal sphincters to remove the tumour while keeping the external sphincter intact and doing that precisely enough to preserve function requires operating in that specific anatomy repeatedly, not the fifth time someone is attempting it.
MIND and RIA-MIND here: Dr. Nayak’s own techniques MIND and RIA-MIND were developed specifically for operating in the narrow pelvis with the precision that low rectal cancer surgery demands and ISR at MACS Clinic is performed within that framework rather than as a standalone procedure disconnected from the broader robotic pelvic surgery experience.
Honest patient selection: ISR is not appropriate for every low rectal cancer and a centre that tells every patient they qualify is not giving honest assessments and at MACS Clinic the conversation about whether ISR fits your tumour location, your sphincter function and your overall fitness happens before surgery not after you’ve already been booked in.
Patients who come to MACS Clinic asking about ISR after being told a permanent stoma was their only option elsewhere frequently find that their case was assessable for sphincter preservation and that the answer they’d been given reflected the limits of the surgical team they saw rather than the limits of what was actually possible for their tumour.Rectal cancer treatment at MACS Clinic covers the full low rectal cancer surgical spectrum from ultra-low anterior resection through ISR where the approach gets matched to what the tumour and the patient’s anatomy actually allow.
What Should You Know Before Getting ISR Surgery in Bangalore?
These are the things worth understanding before committing to ISR for your rectal cancer:
Neoadjuvant therapy first: Most low rectal cancers suitable for ISR benefit from chemoradiation before surgery to shrink the tumour and create the margin that makes sphincter preservation achievable and Dr. Nayak’s plan for ISR starts with the full pre-operative treatment pathway not just the operation.
Function after ISR: Keeping the external sphincter doesn’t automatically mean keeping normal bowel function and low anterior resection syndrome with urgency, frequency and clustering is a real outcome that patients need to understand honestly before choosing ISR over a well-functioning stoma.
Temporary stoma likely: Most ISR operations include a temporary defunctioning stoma to protect the anastomosis while it heals and that gets reversed a few months later in a smaller second operation so a bag immediately after ISR surgery is not the same as a permanent one.
Robotic ISR specifically: ISR performed robotically with the MIND technique in Dr. Nayak’s practice gives the surgeon the magnified view, wristed instruments and precise dissection plane identification in the narrow pelvis that open ISR and even standard laparoscopic ISR cannot reliably replicate for low tumours sitting close to the sphincter.
Whether ISR is achievable for your specific rectal cancer needs your MRI, your staging and a surgeon who has done enough of these to know the difference between a case that genuinely fits and one where the honest answer is that sphincter preservation isn’t safely possible.Colon cancer treatment at MACS Clinic covers the full colorectal surgical spectrum where the ISR conversation sits alongside the full range of colorectal cancer surgical options.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Dr. Sandeep Nayak built MIND and RIA-MIND from operating in the narrow pelvis on low rectal cancer patients repeatedly enough to see where standard technique was leaving outcomes on the table that better dissection could recover. ISR at MACS Clinic isn’t a procedure he offers to patients who ask for it, it’s a procedure he recommends when the case fits and explains why it doesn’t when it doesn’t. 24 years in surgical oncology. Over a thousand robotic cancer surgeries. Chairman of Oncology Services Karnataka. Kidwai Memorial Institute of Oncology alumnus. MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240. If ISR is the right answer for your rectal cancer Dr. Nayak will tell you so and if it isn’t he’ll tell you that too.
Frequently Asked Questions
Where can I get ISR surgery for rectal cancer in Bangalore? ISR for rectal cancer in Bangalore is performed by Prof. Dr. Sandeep Nayak at MACS Clinic Jayanagar using robotic MIND technique, contact plus 91 9482202240.
What is ISR surgery for rectal cancer? Inter-sphincteric resection removes low rectal cancer by dissecting the plane between internal and external anal sphincters preserving the external sphincter and avoiding permanent stoma in selected patients.
Am I suitable for ISR surgery for my rectal cancer? Suitability depends on tumour height from the sphincter, response to neoadjuvant therapy and sphincter function assessment which Dr. Nayak evaluates from your MRI and clinical examination.
How do I book an ISR consultation at MACS Clinic Bangalore? MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240, bring your MRI and all staging scans to the first consultation.
Prof. Dr. Sandeep Nayak at MACS Clinic in Jayanagar Bangalore is consistently where patients across South India end up when they’ve done their research on head and neck cancer surgery properly because 24 years of surgical oncology, trans-oral robotic surgery for oral and base of tongue cancers, neck dissection built into every appropriate operation and a practice that treats the full spectrum of head and neck cancers at real volume is not something you find at many places and certainly not all in the same surgeon.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Head and neck cancer surgery requires preserving function alongside removing the cancer and getting that balance right depends on having operated in this anatomy enough times that the decisions feel instinctive rather than deliberate.”
What Makes Dr. Sandeep Nayak the Best Head and Neck Cancer Surgeon in South India?
These are the things that put Dr. Nayak’s head and neck cancer practice ahead of most alternatives in South India:
Full spectrum: Oral cancer, tongue cancer, oropharyngeal cancer, laryngeal cancer, thyroid cancer, salivary gland tumours, nasopharyngeal cancer and neck metastases are all treated at MACS Clinic rather than a subset of head and neck cancers with the rest referred out to people who may or may not have the same standard.
TORS for oral cancer: Trans-oral robotic surgery removes base of tongue and oropharyngeal tumours through the mouth without any external incision and the robotic camera and wristed instruments working in that space give a view and precision that open surgery through the jaw or neck simply cannot offer for tumours in that location.
RABIT for thyroid: Thyroid cancer removed through armpit and infraclavicular incisions with no cut on the neck is something Dr. Nayak built himself and performs at higher volume than any other centre in South India, available to patients who want their thyroid cancer out without a visible scar on their neck for the rest of their life.
Neck dissection experience: The lymph nodes in the neck are where head and neck cancers spread first and Dr. Nayak’s volume of neck dissections across all head and neck cancer types has built the kind of anatomical familiarity with the neck that means clearing nodes properly while preserving the structures that shouldn’t be touched is something he does from deep experience rather than careful reference to anatomy.
Patients from Chennai, Hyderabad, Kochi, Coimbatore and across South India travel to MACS Clinic in Bangalore for head and neck cancer surgery specifically because the combination of surgical volume, minimally invasive capability and techniques like RABIT and TORS isn’t available at the same level at any single centre closer to where they live.Oral cancer treatment at MACS Clinic covers the full oral cavity and oropharyngeal cancer spectrum where surgical planning starts from what your specific tumour actually needs.
What Head and Neck Cancers Does Dr. Nayak Treat in South India?
These are the head and neck cancer types treated at MACS Clinic under Dr. Nayak’s care:
Oral cavity: Tongue cancer, floor of mouth cancer, buccal mucosa cancer, lip cancer and gingival tumours all treated surgically with clear margins and neck dissection as standard where the staging and clinical picture require it.
Oropharyngeal: Base of tongue cancer, tonsil cancer and soft palate tumours often accessible through TORS rather than conventional open resection which changes what the patient goes through in surgery and what they’re left with in terms of function afterward.
Thyroid and neck: Thyroid cancer with RABIT for eligible patients and conventional thyroidectomy with neck dissection for those where RABIT isn’t appropriate, both performed at a volume that makes the distinction between which fits your case something Dr. Nayak can answer from experience rather than from guidelines.
Laryngeal and salivary: Laryngeal cancer, parotid tumours and submandibular gland cancers treated surgically with the function preservation approach that distinguishes specialist surgical oncology from general surgery encountering these cases occasionally.
Whether your specific head and neck cancer fits what MACS Clinic does and what approach your tumour location and stage call for is a conversation for a consultation rather than a website and Dr. Nayak will tell you honestly what the options are for your case.Thyroid cancer treatment at MACS Clinic covers thyroid cancer specifically as one of the primary head and neck cancer types where RABIT gives patients an option no other centre in South India offers at the same volume.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Oral cancer. Tongue cancer. Oropharyngeal cancer. Thyroid cancer. Laryngeal cancer. Salivary gland tumours. All of them at real volume for 24 years. TORS built into the practice. RABIT built here. Neck dissection done repeatedly enough that it’s familiarity not caution. Over a thousand robotic cancer surgeries. Chairman of Oncology Services Karnataka. Kidwai Memorial Institute of Oncology alumnus. MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240. Patients from across South India who ask the right questions about head and neck cancer surgery consistently end up here.
Frequently Asked Questions
Who is the best head and neck cancer surgeon in South India? Prof. Dr. Sandeep Nayak at MACS Clinic Jayanagar Bangalore treats the full spectrum of head and neck cancers with 24 years of experience, TORS and RABIT available, contact plus 91 9482202240.
Does Dr. Sandeep Nayak perform trans-oral robotic surgery for head and neck cancer? Yes, TORS for base of tongue and oropharyngeal cancers is available at MACS Clinic Bangalore giving patients robotic oral cancer surgery without external incisions.
Which head and neck cancers does Dr. Sandeep Nayak treat at MACS Clinic? Oral cavity, tongue, oropharyngeal, thyroid, laryngeal, salivary gland and neck metastases are all treated at MACS Clinic as part of the full head and neck cancer surgical programme.
How do I book a head and neck cancer consultation at MACS Clinic Bangalore? MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240, bring all imaging and biopsy reports to the first appointment.
For mouth cancer treatment in Bangalore MACS Clinic in Jayanagar is where patients who’ve done their research tend to end up because Prof. Dr. Sandeep Nayak has 24 years of surgical oncology experience, performs trans-oral robotic surgery for oral and base of tongue cancers and builds every treatment plan from the patient’s actual imaging and pathology rather than from a protocol written before anyone looked at the scans.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Mouth cancer surgery done properly means removing the tumour with clear margins while preserving as much speech and swallowing function as possible and that balance requires a surgeon who has done this at real volume rather than occasionally.”
What Makes MACS Clinic the Right Choice for Mouth Cancer Treatment in Bangalore?
These are the things that set MACS Clinic apart for mouth cancer treatment specifically:
Surgical volume: Dr. Nayak operates on oral cancers at real volume which means the anatomical familiarity, the ability to read what’s on the imaging before entering the theatre and the judgment about margin adequacy versus function preservation that comes from doing this repeatedly rather than occasionally.
TORS available: Trans-oral robotic surgery for base of tongue and oropharyngeal cancers removes tumours through the mouth without external incisions and the robotic camera and wristed instruments give access and precision in that location that open surgery through an external incision genuinely cannot match.
Neck dissection integrated: Mouth cancer spreads to neck lymph nodes early and Dr. Nayak builds neck dissection into the surgical plan from the start rather than treating it as a separate procedure the patient has to go through again after the primary surgery is done.
Function preservation: Getting clear margins without unnecessarily sacrificing speech and swallowing function is what separates surgical oncology from general surgery with a cancer diagnosis and it’s where the experience of a surgeon who has operated on oral cancers repeatedly shows up most directly in what patients end up with after treatment.
Patients with mouth cancer who come to MACS Clinic in Bangalore consistently say the conversation about their case was more specific, more honest and more focused on what their actual imaging showed than consultations they’d had elsewhere before finding Dr. Nayak.Oral cancer treatment at MACS Clinic covers the full spectrum of mouth and oral cavity cancers where surgical planning is built from what the case actually requires.
What Should Mouth Cancer Patients Expect at MACS Clinic Bangalore?
These are the things patients coming to MACS Clinic for mouth cancer treatment should know before their first consultation:
Honest staging assessment: Dr. Nayak looks at the imaging himself and tells you honestly what stage your mouth cancer is at, whether surgery alone covers it or whether radiation and chemotherapy are part of the plan and what the realistic outcomes look like for your specific case.
Surgical approach explained: Whether your mouth cancer needs conventional resection, trans-oral robotic surgery or a combined approach gets explained in terms of what your tumour location, size and pathology actually call for rather than what the centre finds most convenient to offer.
Reconstruction discussed: Mouth cancer surgery sometimes requires reconstruction of the oral cavity and that conversation, what reconstruction involves, what it means for speech and swallowing and what recovery looks like, happens before surgery at MACS Clinic not as a surprise during the post-operative period.
Adjuvant treatment coordination: Dr. Nayak coordinates with radiation and medical oncology for patients who need post-operative treatment so that the transition from surgery to adjuvant therapy is planned rather than something the patient has to organise themselves after being discharged from surgical care.
Whether MACS Clinic is the right place for your specific mouth cancer case depends on your staging, your tumour location and a consultation where Dr. Nayak can look at what you’ve actually got.Head and neck cancer treatment at MACS Clinic covers oral, tongue, oropharyngeal and other mouth cancers where surgical precision and function preservation are both part of what the treatment aims for.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
24 years in surgical oncology. Trans-oral robotic surgery for oral and base of tongue cancers. Neck dissection built into every appropriate head and neck operation. Over a thousand robotic cancer surgeries across cancer types. RABIT, MIND and RIA-MIND developed here. Chairman of Oncology Services Karnataka. Kidwai Memorial Institute of Oncology alumnus. MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240. Mouth cancer surgery done properly means the right margins and the best possible function on the other side of it and that’s what Dr. Nayak’s practice is built around.
Frequently Asked Questions
What is the best hospital for mouth cancer treatment in Bangalore? MACS Clinic Jayanagar Bangalore under Prof. Dr. Sandeep Nayak offers oral cancer surgery including trans-oral robotic surgery and neck dissection with 24 years of surgical oncology experience, contact plus 91 9482202240.
Does Dr. Sandeep Nayak perform trans-oral robotic surgery for mouth cancer? Yes, TORS for base of tongue and oropharyngeal cancers is available at MACS Clinic Bangalore giving patients access to robotic oral cancer surgery without external incisions.
How is mouth cancer treated at MACS Clinic Bangalore? Through surgical resection with clear margins, neck dissection when indicated, trans-oral robotic surgery where appropriate and coordination with radiation and medical oncology for adjuvant treatment.
How do I book a mouth cancer consultation at MACS Clinic Bangalore? MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240, bring all imaging and biopsy reports to the first consultation.
If the surgeon in your city doesn’t do your specific procedure at real volume, doesn’t offer minimally invasive surgery for your cancer type or gave you a treatment plan that felt like it was built for the average case rather than yours specifically then yes travelling to Bangalore for cancer surgery is worth it and the patients who make that decision and then sit across from Dr. Sandeep Nayak at MACS Clinic consistently say the gap between what they were offered locally and what they found here was larger than they expected.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Patients who travel to Bangalore for cancer surgery are usually the ones who asked the right questions locally and didn’t get satisfying answers and that instinct to look further is usually worth following.”
When Does It Make Sense to Travel to Bangalore for Cancer Surgery?
These are the situations where travelling to Bangalore for cancer surgery is worth the effort:
Low local volume: If the surgeon in your city does your specific procedure ten or fifteen times a year and a specialist in Bangalore does it fifty or a hundred times the outcomes data says that difference matters and travelling is genuinely the better decision for your cancer not just a preference.
No minimally invasive option: If you’ve been told open surgery is the only option for your cancer type without a specific clinical reason related to your tumour being given then a second opinion from a centre doing laparoscopic and robotic surgery for that cancer type at real volume is worth getting before you agree to anything.
Complex or rare case: Rectal cancer requiring sphincter preservation, scarless thyroid surgery, HIPEC for peritoneal spread, inter-sphincteric resection, these are procedures where the difference between a centre doing them occasionally and one doing them regularly at genuine volume is the difference between having them done properly and having them done with the outcome a less experienced team is capable of producing.
Something didn’t feel right: If you left a consultation with a treatment plan you didn’t fully understand, a surgeon who seemed to be fitting your case into a standard protocol rather than building a plan from your specific scans or a recommendation that didn’t sit right with you that instinct deserves a second opinion before surgery rather than after it.
Travelling from Chennai, Mumbai, Hyderabad, Delhi or anywhere else in India to Bangalore for a consultation at MACS Clinic costs less than the difference between a surgery done properly and one that requires a re-operation.Robotic cancer surgery at MACS Clinic is what patients from other Indian cities are travelling to Bangalore for and the reason they come is specific rather than general.
What Do Patients From Other Cities Need to Know Before Travelling to Bangalore?
These are the practical things worth sorting out before you make the trip:
Online consultation first: Call plus 91 9482202240 or reach out online, share your scans, pathology and treatment history remotely and have an online consultation with Dr. Nayak before travelling so you know whether your case fits what MACS Clinic does before you book a train or a flight.
Bring everything: Scans, biopsy reports, blood tests, previous surgery notes, referral letters, all of it because Dr. Nayak looks at the actual imaging himself and the difference between a consultation with complete prior records and one without them is the difference between a treatment plan and a list of investigations to go and get done before one can be made.
Plan for the full process: If your consultation leads to surgery at MACS Clinic plan a stay that covers pre-operative workup, the procedure itself and enough initial recovery to travel home safely rather than booking a return ticket for three days after surgery.
Remote follow-up after: Patients from other cities who’ve had surgery at MACS Clinic manage post-operative follow-up through online consultations with Dr. Nayak and their local physician which makes the ongoing care after surgery practical rather than requiring repeated trips back to Bangalore.
Whether travelling to Bangalore for cancer surgery is the right call for your specific case is a question an online consultation with Dr. Nayak can answer before you commit to the journey rather than after you’ve already made it.Laparoscopic cancer surgery at MACS Clinic covers the full minimally invasive spectrum for patients travelling from other Indian cities who want surgical options their local centre isn’t offering.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
The patients who travel from other Indian cities to MACS Clinic in Jayanagar Bangalore did their research, asked the right questions locally and decided the answer was somewhere else. 24 years in surgical oncology. Over a thousand robotic cancer surgeries. RABIT, MIND and RIA-MIND built here. Chairman of Oncology Services Karnataka. Kidwai Memorial Institute of Oncology alumnus. Monday to Saturday 3pm to 6:30pm. Contact plus 91 9482202240. Start with an online consultation and find out whether travelling makes sense for your case before you decide it doesn’t.
Frequently Asked Questions
Should I travel to Bangalore for cancer surgery from another city? If your local surgeon doesn’t do your procedure at real volume, doesn’t offer minimally invasive surgery or gave you a plan that felt generic rather than specific then yes a consultation in Bangalore is worth the trip.
How do I arrange a consultation at MACS Clinic from another city? Call or WhatsApp plus 91 9482202240, share your reports and scans remotely and arrange an online consultation with Dr. Nayak before travelling to Bangalore.
How long do patients from other cities need to stay in Bangalore for surgery? Long enough for pre-operative workup, surgery and initial recovery before travelling home, typically two to three weeks depending on the procedure and how quickly recovery progresses.
Can post-operative follow-up be done remotely after surgery at MACS Clinic? Yes, patients from other cities manage follow-up through online consultations with Dr. Nayak and coordination with their local physician after returning home.
Dr. Sandeep Nayak has been featured in Forbes India as a recognised surgical oncologist in India and that kind of feature tends to happen not because someone submitted an application for it but because a publication looking at who is actually moving the needle in a field keeps arriving at the same name when they talk to the right people and ask the right questions about who is doing something that didn’t exist before they started doing it.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Recognition in publications like Forbes means something when it reflects what the surgical oncology community already knows rather than what a PR campaign managed to put in front of an editor.”
What Has Forbes India Recognised About Dr. Sandeep Nayak?
These are the things that Forbes India’s recognition of Dr. Nayak reflects about his standing in surgical oncology:
Original innovation: Forbes features in healthcare tend to land on people who built something rather than people who adopted something and Dr. Nayak’s development of RABIT, MIND and RIA-MIND gave a publication looking at Indian surgical oncology something genuinely original to write about.
Robotic surgery pioneer: Getting into robotic cancer surgery over 15 years ago in India before most centres had committed to it and building a practice at real volume from that early start is the kind of trajectory that makes someone a relevant subject for a publication tracking who shaped a field rather than who followed it.
Patient impact: Forbes India coverage of surgical oncologists reflects what patients are experiencing in outcomes rather than what doctors are saying about themselves and a practice where international patients fly in specifically for procedures that aren’t available at the same level anywhere closer to where they live generates the kind of impact that publications notice.
Building the evidence base: Developing techniques and documenting their outcomes for the Indian patient population rather than importing and adapting techniques developed elsewhere gives Dr. Nayak’s contribution to surgical oncology in India a specific character that distinguishes it from high quality practice that doesn’t produce new knowledge.
Forbes India recognition sits in the same category as the other forms of recognition Dr. Nayak’s career has generated, it came from what the practice produced rather than from efforts to generate it and that’s generally the kind that reflects something real about a career rather than something managed.Robotic cancer surgery at MACS Clinic is the practice that Forbes India was writing about when it featured Dr. Nayak rather than a profile built for the purpose of being featured.
What Does Forbes India Recognition Mean for Patients Choosing a Cancer Surgeon?
These are the reasons Forbes India coverage of a surgical oncologist matters and the reasons it doesn’t:
Validation not selection: A Forbes India feature on a surgical oncologist validates that someone has built something worth writing about but it doesn’t tell you whether their specific expertise matches your specific cancer and patients should use it as confirmation of what their own research has already found rather than as the starting point of that research.
Volume still the question: Being featured in Forbes India doesn’t tell you how many cases of your specific procedure the surgeon does per year and that number is still the most important single piece of information a patient can gather before choosing a cancer surgeon regardless of what publications have written about them.
What got featured: Understanding what specifically Forbes India recognised Dr. Nayak for, his technique development, his robotic surgery volume, his outcomes in specific cancer types, is more useful to a patient than the fact of the feature itself because it tells you which part of his practice the coverage was about.
Consistent recognition pattern: A surgeon featured in Forbes India, chairing oncology services across Karnataka and developing techniques that other surgeons travel to learn is showing a consistent pattern of external validation across different types of recognition that points toward something real rather than a single high-profile moment.
Whether the career Forbes India recognised is the right match for your specific cancer case is a question worth exploring in a consultation rather than assuming because a publication wrote well about someone they’re automatically the right surgeon for every case that walks in.Thyroid cancer treatment at MACS Clinic is one of the areas Dr. Nayak has been recognised for specifically given his development of RABIT scarless thyroid surgery.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Featured in Forbes India. Chairman of Oncology Services Karnataka. Developer of RABIT, MIND and RIA-MIND. Over a thousand robotic cancer surgeries. 24 years in surgical oncology. Kidwai Memorial Institute of Oncology alumnus. International patients flying in specifically for procedures they couldn’t find at the same level anywhere closer. MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240. The recognition is consistent across sources because what it’s recognising is consistent across cases.
Frequently Asked Questions
Is Dr. Sandeep Nayak mentioned in Forbes India? Yes, Dr. Sandeep Nayak has been featured in Forbes India as a recognised surgical oncologist known for developing RABIT, MIND and RIA-MIND and his robotic cancer surgery practice at MACS Clinic Bangalore.
What was Dr. Sandeep Nayak featured in Forbes India for? His development of original surgical techniques including RABIT scarless thyroid surgery and MIND and RIA-MIND for pelvic cancer surgery and his robotic surgical oncology practice in India.
Does Forbes India recognition mean Dr. Sandeep Nayak is the right surgeon for my cancer? Forbes India validates the track record but patients should confirm the surgeon’s specific volume and expertise in their cancer type through a consultation before making any treatment decision.
How do I book a consultation with Dr. Sandeep Nayak at MACS Clinic? MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240.
Dr. Sandeep Nayak’s primary practice is MACS Clinic in Jayanagar Bangalore and that’s genuinely the most important answer to this question because MACS Clinic is where he sees patients, where the consultations happen, where RABIT and MIND and RIA-MIND were built and where someone calling plus 91 9482202240 on a Monday afternoon will actually reach the practice that operates under his name.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “MACS Clinic is built around doing surgical oncology properly for each patient rather than efficiently for large numbers and that difference in how a practice is structured shows up in what patients experience when they’re in it.”
Which Hospital or Clinic Is Dr. Sandeep Nayak Associated With?
These are the things worth understanding about where Dr. Nayak actually practices:
MACS Clinic: Jayanagar Bangalore, this is the primary practice, consultations happen here, pre-operative planning happens here, follow-up happens here and the whole surgical oncology programme that Dr. Nayak has built over 24 years lives here rather than inside a large hospital system somewhere.
Specialist practice: A dedicated surgical oncology practice is a different thing from a large corporate hospital with an oncology department and the difference shows up in consultation quality, in how much of the surgeon’s attention is actually on your case and in whether the person you see first is Dr. Nayak or someone presenting your notes to him.
Techniques stay here: RABIT, MIND and RIA-MIND are at MACS Clinic because Dr. Nayak built them here and the team and experience that makes those techniques work properly hasn’t been dispersed across a hospital system where the robotic programme competes with fifteen other departments for theatre slots and resources.
Hospital for surgery: Complex procedures requiring ICU support or major robotic infrastructure happen at associated hospitals in Bangalore with the right equipment but the consultation, the treatment plan and the post-operative care planning all stay centred at MACS Clinic rather than disappearing into a large institution.
Patients come to MACS Clinic first and the conversation there is where everything starts rather than after someone has already decided what treatment will happen based on a referral letter nobody sat down and properly read.Robotic cancer surgery at MACS Clinic is the starting point for understanding what Dr. Nayak’s practice offers rather than which hospital name is on any given piece of paperwork.
What Makes MACS Clinic Different From a Large Hospital?
These are the things patients notice when they compare MACS Clinic to large corporate hospitals they visited before ending up here:
He actually sees you: Not a registrar, not a junior collecting history, Dr. Nayak looks at your scans himself and that sounds like it should be standard but anyone who has been to a busy hospital outpatient department knows it absolutely isn’t.
Your case gets time: At MACS Clinic the consultation lasts as long as your cancer case needs it to rather than ending when a slot timer runs out and the next patient is already sitting outside wondering when their turn starts.
No queue pressure: Large hospitals move patients through efficiently because they have to and the effect that has on how much anyone is actually thinking about your specific situation rather than the next twenty cases is something patients feel even when they can’t name exactly what was wrong with the consultation they just left.
Same people throughout: Consultation, surgery, follow-up, Dr. Nayak’s practice rather than different departments of a large institution that have technically been copied on your file but haven’t read it.
The structure of where a surgeon practises is the structure of what your cancer treatment actually feels like from the first phone call to the last follow-up and MACS Clinic was built to make that experience look the way it should rather than the way a large hospital system requires it to look.Laparoscopic cancer surgery at MACS Clinic covers the full minimally invasive spectrum inside a practice built specifically around doing this right.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
MACS Clinic Jayanagar Bangalore. That’s where it happens. 24 years in surgical oncology. Over a thousand robotic cancer surgeries. RABIT built here not borrowed. MIND built here. RIA-MIND built here. Chairman of Oncology Services Karnataka. Kidwai Memorial Institute of Oncology alumnus. Monday to Saturday 3pm to 6:30pm. Plus 91 9482202240. The hospital association matters less than where the surgeon actually practices and what that practice was built to do for the people who come through the door.
Frequently Asked Questions
Which hospital is Dr. Sandeep Nayak associated with? MACS Clinic Jayanagar Bangalore is his primary practice, Monday to Saturday 3pm to 6:30pm, contact plus 91 9482202240.
Where does Dr. Sandeep Nayak perform surgery? Complex surgery happens at associated hospitals in Bangalore with the right infrastructure but consultation and care planning stays at MACS Clinic.
How is MACS Clinic different from a large hospital? Dr. Nayak sees patients himself, cases get the time they need and care is continuous rather than fragmented across departments that have technically been cc’d on your file.
How do I book an appointment with Dr. Sandeep Nayak? Call or WhatsApp plus 91 9482202240, MACS Clinic Jayanagar Bangalore, Monday to Saturday 3pm to 6:30pm.
Dr. Sandeep Nayak, a board-certified surgical oncologist (M.ch ., D.N.B.), specializes in minimally invasive cancer surgery, including robotic and laparoscopic techniques.