Robotic vs Laparoscopic Surgery for Ovarian Cancer?
This comparison applies to a narrower group than most patients expect, early stage, apparently confined ovarian cancer only. Advanced disease requiring extensive debulking still needs open surgery. Within that early stage indication, robotic surgery offers three dimensional vision and wristed instrumentation, compared to the two dimensional view and rigid instruments of laparoscopic surgery. Neither has shown a clear survival advantage over the other in ovarian cancer specifically. The real difference here is technical, not oncological.
According to Dr. Sandeep Nayak, Surgical Oncologist in India, “The first thing patients need to understand is scope. This comparison only applies to early, confined ovarian cancer. Advanced disease with extensive spread still requires open surgery for adequate debulking. Within early stage cases, robotic surgery gives me better vision and more precise instrument control than standard laparoscopy. But I want to be honest, there is no strong evidence that this technical advantage translates into better survival for ovarian cancer specifically. The staging itself matters more than the platform.”
Diagnosed with early stage ovarian cancer and weighing surgical options?
Where Does This Comparison Actually Apply?
Understanding the scope of this comparison matters more than the comparison itself.
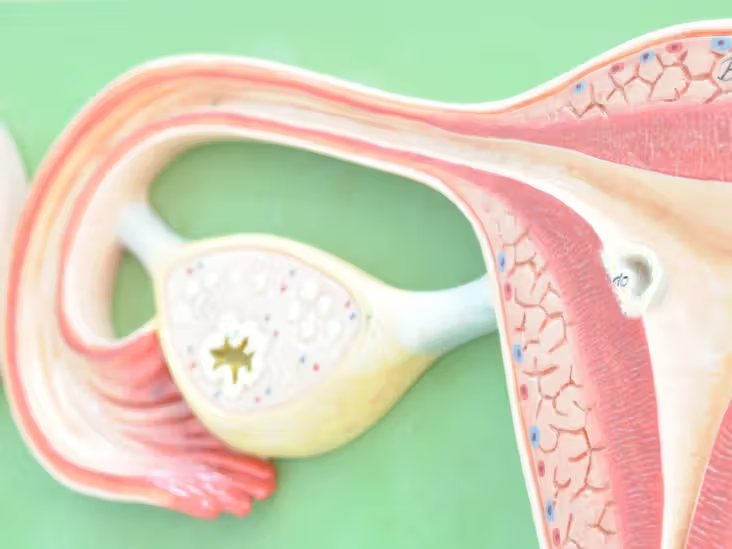
- Early stage only : This choice applies to disease that appears confined to the ovary on imaging, not to advanced or bulky disease.
- Advanced disease excluded : Cancer requiring extensive debulking across the peritoneal surfaces still needs open surgery for complete visualisation and access.
- Staging concerns : Minimally invasive approaches to ovarian cancer carry more caution than in some other gynaecological cancers, given concerns about missing occult spread.
- A narrow but real question : For the right early stage case, both platforms are legitimate minimally invasive options worth comparing directly.
This distinction shapes how surgical planning fits within broader ovarian cancer treatment, where stage decides the surgical approach before technique is even considered.
Robotic or Laparoscopic: How Do They Compare?
Here is how the two platforms line up within their shared, early stage indication.
|
Feature |
Robotic |
Laparoscopic |
|
Visualisation |
Three dimensional |
Two dimensional |
|
Instrument movement |
Wristed, more degrees of freedom |
Rigid, limited articulation |
|
Ergonomics |
Console based, seated |
Standing, less ergonomic |
|
Survival outcomes |
No clear advantage shown |
No clear advantage shown |
|
Applies to |
Early stage disease only |
Early stage disease only |
|
Learning curve |
Often considered gentler |
Steeper for complex tasks |
- Vision and precision : The three dimensional view and wristed movement give robotic surgery a technical edge for fine dissection and suturing.
- Similar oncological result : For appropriately selected early stage cases, staging accuracy and outcomes are comparable between the two approaches.
- Not a survival decision : Choosing between them is reasonably a matter of surgeon experience and available technology, not expected cancer control.
- The real decision point : Whether minimally invasive surgery applies at all matters far more than which platform is chosen within it.
This is directly relevant to how early stage ovarian cancer is approached surgically once the disease has been properly staged.
Why Choose Dr. Sandeep Nayak for Ovarian Cancer Surgery?
Dr. Sandeep Nayak is a surgical oncologist with 24 years of experience and a fellowship in laparoscopic and robotic onco-surgery. His approach to ovarian cancer surgery begins with an honest assessment of stage and resectability, since that determines whether minimally invasive surgery is appropriate at all before robotic versus laparoscopic technique becomes relevant. This means offering both platforms and selecting based on the individual case rather than a fixed preference.
The more consequential decision in ovarian cancer surgery is not robotic versus laparoscopic, it is confirming the disease genuinely suits a minimally invasive approach in the first place. Getting that staging judgement right protects against understaging advanced disease through an inappropriately limited operation. Within the correct early stage indication, either platform in experienced hands can deliver an equivalent oncological result.
Frequently Asked Questions
Is robotic surgery better than laparoscopic for ovarian cancer?
No clear survival advantage exists between them. The difference is mainly technical.
Can minimally invasive surgery treat advanced ovarian cancer?
No. Advanced disease requiring debulking still needs open surgery.
Which ovarian cancers suit minimally invasive surgery?
Early stage disease that appears confined to the ovary on imaging.
What advantage does robotic surgery offer over laparoscopic?
Three dimensional vision and wristed instruments, offering technical rather than survival benefits.
References
- Minimally invasive surgery for early stage ovarian cancer — National Library of Medicine
- Robotic versus laparoscopic gynaecologic oncology outcomes — National Library of Medicine
Disclaimer: This blog is for informational and educational purposes only and is not a substitute for professional medical advice or diagnosis.