What Is Multidisciplinary Cancer Care ?
Cancer treatment is too complex for one clinician to plan alone. Multidisciplinary cancer care puts surgical oncologists, medical oncologists, radiation oncologists, pathologists and radiologists in the same room to review each case before any treatment is confirmed. What comes out of that process is consistently more accurate and better sequenced than what one specialist working independently would produce for the same patient.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India,
“The tumour board is where the most important decisions in cancer care actually get made. Complex cases rarely have one obvious answer and getting multiple specialist views on the same findings consistently changes what gets recommended.”
Want your cancer case reviewed by a full multidisciplinary team?
What Actually Happens at a Tumour Board?
The tumour board is not a meeting where a plan gets explained to a group. It is where the plan gets built, challenged and finalised by specialists reviewing the same evidence together.
- Direct Review Not Summaries: Biopsy slides, imaging and clinical history are presented to the full team in the meeting itself. The radiologist reads the scans, the pathologist reviews the tissue and the oncologists contribute their clinical assessment before any conclusion is reached.
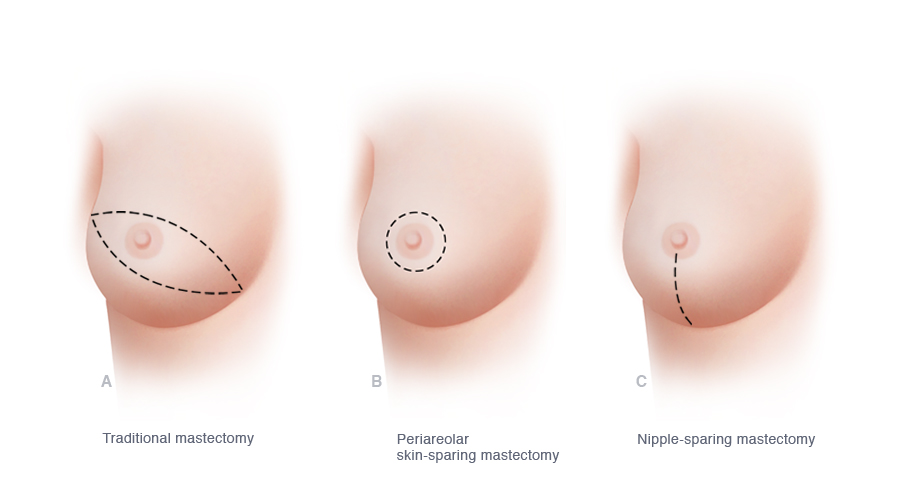
- Sequence Gets Decided Here: Whether surgery or chemotherapy comes first, which drug regimen fits the receptor profile, whether radiation runs concurrently or after the operation. Breast cancer treatment decisions including surgery type are among those most frequently modified after board discussion at high-volume centres.
- Difficult Cases Get Resolved: Borderline resectable tumours, conflicting staging findings and unusual presentations are where tumour boards add the most clinical value. A single specialist seeing the same case would reach a conclusion faster but not necessarily the right one.
- Plans Get Revisited: After neoadjuvant chemotherapy, after surgery, when new findings emerge. The board reassesses at each decision point rather than locking a plan in at the first meeting and following it regardless of how the disease has actually responded.
The patient receives a clear explanation of what was decided and why rather than being handed a treatment plan without any context behind it.
Why Does It Produce Better Results Than Single-Specialist Care?
The evidence runs across staging accuracy, treatment selection and patient outcomes at centres that have implemented multidisciplinary care properly.
- Cross-Checking Catches More: When a radiologist, pathologist and surgeon review the same case without knowing what the others found, findings that one clinician might not flag tend to be identified by another. In cancers where imaging interpretation and pathology grading directly influence treatment this catching process changes outcomes in ways that matter.
- Plans Change After Review: A meaningful proportion of cancer cases arrive at tumour board with a treatment plan that gets modified after specialist review. Those changes represent clinical value the patient would not have received through a single-specialist pathway regardless of that clinician’s experience.
- Timing Gets Coordinated: Surgery, chemotherapy and radiation need to run in the right order and start at the right time relative to each other. Robotic cancer surgery results improve when the medical oncology and radiation teams are aligned on timing before the operation rather than learning the plan independently afterward.
- More Options Surface: High-volume multidisciplinary centres identify clinical trial eligibility and newer protocol access that single-specialist pathways rarely raise. Patients seen only by one clinician in one department often don’t know options exist that a tumour board would have flagged immediately.
Multidisciplinary care is the standard at every centre that treats cancer at meaningful volume, and for more on what cancer surgery involves within this framework, our blog on cancer surgery covers this in detail.
Why Choose Dr. Sandeep Nayak for Cancer Treatment ?
Dr. Sandeep Nayak brings 24 years of surgical oncology experience, DNB qualifications in Surgical Oncology and General Surgery and a fellowship in Laparoscopic and Robotic Onco-Surgery to every cancer case reviewed through tumour board at KIMS Hospital, Bangalore. He heads Oncology Services across Karnataka with originator credits for RABIT, MIND and L-VEIL techniques and over 25 published clinical studies. Every patient seen here has their case reviewed through a full multidisciplinary tumour board before any treatment decision is finalised. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
Who sits on a multidisciplinary cancer tumour board?
Surgical oncologist, medical oncologist, radiation oncologist, pathologist and radiologist with additional specialists added based on cancer type.
How often does a tumour board meet?
Most high-volume cancer centres hold weekly tumour board meetings with cases presented before treatment begins and at key decision points.
Does every cancer patient need a tumour board review?
Complex and locally advanced cases benefit most though high-volume centres review all cases as standard practice rather than exception.
How does a patient benefit from multidisciplinary cancer care?
Treatment plans reviewed by multiple specialists are more accurate, better timed and more likely to reflect current clinical evidence than single-specialist decisions.
References
-
- National Cancer Institute — Multidisciplinary Cancer Care
- National Institutes of Health — Tumour Board Review in Oncology
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.