
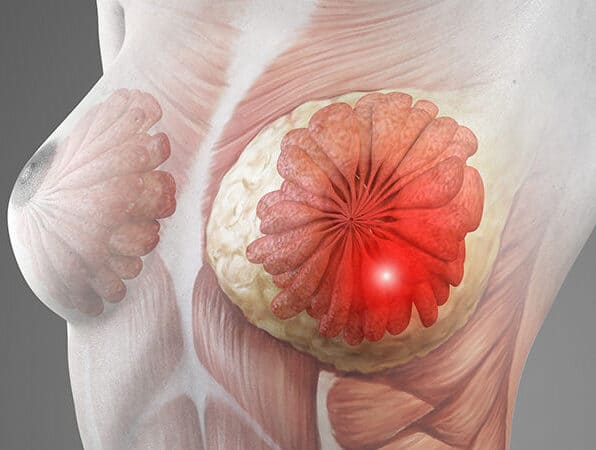
Inflammatory breast cancer is one of the rarest but most aggressive forms of breast cancer. It doesn’t usually present as a lump instead the breast becomes red, warm, swollen and heavy, which is why it gets mistaken for mastitis or an infection far more often than any other breast cancer type. That misdiagnosis costs time, and with IBC time genuinely matters more than with most other breast cancers.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India,
“IBC is dangerous precisely because it doesn’t look like what most people expect breast cancer to look like the absence of a lump doesn’t mean the absence of cancer, and any breast that’s suddenly red, swollen and warm needs urgent assessment.”
Breast changes that don’t feel right and aren’t responding to antibiotics?
How Is Inflammatory Breast Cancer Different From Other Types?
IBC behaves differently from typical breast cancer in almost every clinically relevant way presentation, spread pattern and treatment sequence all diverge from the standard picture.
- No Lump Present: Most breast cancers announce themselves through a palpable mass IBC spreads through the skin lymphatics instead, causing the overlying skin to thicken into an orange-peel texture called peau d’orange that’s pathognomonic for this diagnosis.
- Rapid Progression: Symptoms appear and worsen over weeks rather than months, and breast cancer treatment for IBC always starts with chemotherapy rather than surgery because operating before systemic treatment rarely produces the outcomes the patient needs.
- Already Stage 3 at Diagnosis: By the time IBC is confirmed the disease is classified as at least locally advanced the cancer has already involved dermal lymphatics which means it has spread beyond a single tumour site even before staging scans are completed.
- Mistaken for Infection: The redness, warmth and swelling look identical to mastitis and many patients complete a full course of antibiotics before anyone considers a cancer diagnosis the key difference is that infection improves with antibiotics and IBC doesn’t.
Getting to a correct diagnosis quickly is what determines whether the treatment plan can stay ahead of the disease or ends up chasing it.
How Is IBC Diagnosed and Treated?
Diagnosis requires clinical suspicion first imaging and biopsy confirm it but a clinician has to consider the possibility before any test gets ordered.
- Skin Punch Biopsy: Because there’s often no discrete lump to sample, a punch biopsy of the thickened skin confirms cancer cells in the dermal lymphatics and establishes the IBC diagnosis when clinical presentation already suggests it strongly.
- Staging Scans: PET-CT is preferred for IBC staging because the disease spreads early and conventional CT sometimes underestimates nodal and distant involvement in a cancer that moves through lymphatic channels rather than forming a contained mass.
- Neoadjuvant Chemotherapy First: Surgery never opens an IBC treatment plan chemotherapy comes first to reduce disease burden and assess how the cancer responds to systemic treatment before the surgical team considers what operation is appropriate.
- Modified Radical Mastectomy: When chemotherapy has achieved sufficient response, robotic cancer surgery or conventional modified radical mastectomy removes the breast and axillary nodes, followed by radiation to the chest wall because breast-conserving surgery isn’t appropriate for IBC regardless of how well the cancer has responded.
Treatment for IBC is long, intensive and requires a team that understands the condition it’s not managed the same way as standard breast cancer, and for more on breast cancer surgery options overall, our blog on breast reconstruction covers post-surgical considerations in detail.
Why Choose Dr. Sandeep Nayak for Breast Cancer Treatment ?
Dr. Sandeep Nayak brings 24 years of surgical oncology experience, DNB qualifications in Surgical Oncology and General Surgery and a fellowship in Laparoscopic and Robotic Onco-Surgery to complex breast cancer cases including inflammatory presentations. He heads Oncology Services across Karnataka and leads breast cancer surgery at KIMS Hospital, Bangalore, with originator credits for RABIT and over 25 published clinical studies. Patients with suspected IBC or unusual breast cancer presentations that haven’t been properly assessed elsewhere are seen here with every decision going through tumour board review. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
Can inflammatory breast cancer be mistaken for an infection?
Yes, it frequently is the key difference is that IBC doesn’t improve with antibiotics the way mastitis does.
Is inflammatory breast cancer always treated with chemotherapy first?
Yes, neoadjuvant chemotherapy always precedes surgery in IBC regardless of how early the diagnosis is made.
diagnosis is made. Can lumpectomy be used for inflammatory breast cancer?
No, breast-conserving surgery is not appropriate for IBC modified radical mastectomy followed by radiation is standard.
How fast does inflammatory breast cancer progress?
Symptoms typically develop and worsen over weeks rather than months, making early assessment urgent.
References
-
- National Cancer Institute — Inflammatory Breast Cancer
- National Institutes of Health — IBC Diagnosis and Treatment
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.
