What Is Sentinel Lymph Node Biopsy in Breast Cancer ?
Before treating breast cancer properly, the surgical team needs to know whether it has spread to the lymph nodes under the arm. Sentinel lymph node biopsy answers that question by checking just the first node cancer would reach — if that one’s clear, the others almost certainly are too. It’s replaced routine full node removal for most early-stage patients and that change has made a real difference to how women recover from breast cancer surgery.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India,
“Sentinel node biopsy gives us the nodal information we need while sparing patients from complications they don’t need to face if their nodes are clear.”
Need to understand what sentinel node biopsy means for your treatment?
How Does the Procedure Work in Practice?
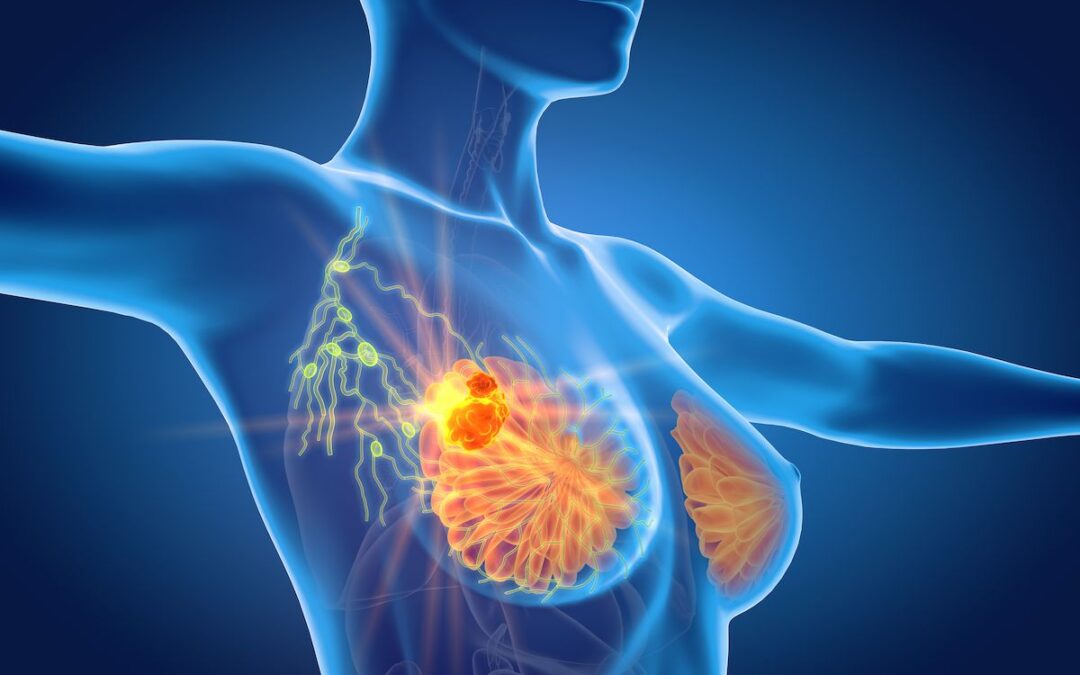
Finding the sentinel node isn’t guesswork the team uses a tracer that follows the same path cancer cells would take from the tumour.
- Tracer First: A radioactive substance, blue dye or both get injected near the tumour before surgery and travel through the lymphatic channels until they collect in the first draining node, which the surgeon then identifies and removes during the operation.
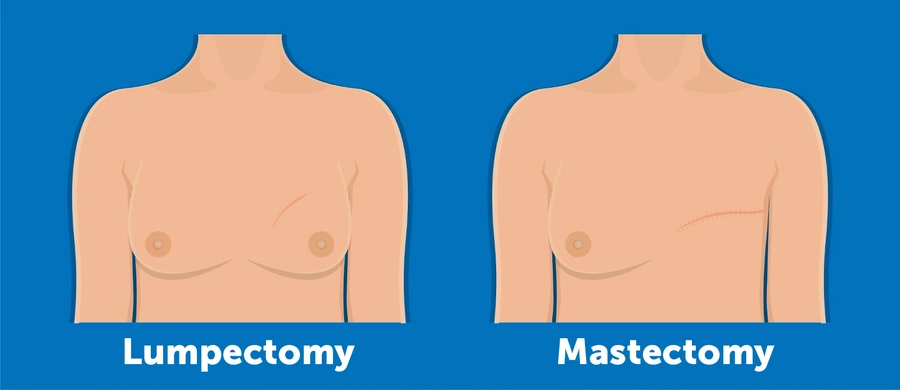
- Same Session: The biopsy happens during the same operation as breast cancer treatment lumpectomy or mastectomy so there’s no separate procedure, no second anaesthetic and no meaningful addition to the patient’s recovery time.
- Immediate Pathology: The removed node goes straight to the lab during surgery and if cancer cells are found the team decides in real time whether to take more nodes out or manage the axilla through radiation after recovery.
- Clear Node Outcome: When pathology confirms no cancer, the remaining axillary nodes stay exactly where they are and the patient avoids the arm swelling, restricted movement and chronic discomfort that comes with removing lymph nodes that weren’t involved.
The nodal result feeds directly into staging, chemotherapy decisions and radiation planning it’s one piece of information that changes multiple downstream treatment decisions.
Why Does Nodal Status Matter This Much?
Whether cancer has reached the lymph nodes is one of the single most important clinical facts in early breast cancer management.
- Changes the Stage: A positive sentinel node moves the patient from node-negative to node-positive staging immediately, and that shift often brings adjuvant chemotherapy into a plan where it wasn’t being considered before the biopsy result came back.
- Avoids Unnecessary Surgery: Full axillary clearance used to be routine regardless of node status most patients never needed it and spent years dealing with lymphoedema that could have been avoided with a targeted approach from the start.
- When Nodes Are Positive: The decision between full axillary dissection and axillary radiation is made based on how many nodes are involved and what the overall treatment plan looks like, because both approaches have similar oncological outcomes in selected patients.
- High Accuracy: Experienced surgical centres achieve correct nodal identification in over 95% of cases and robotic cancer surgery programmes routinely integrate sentinel node biopsy into minimally invasive breast operations without adding complexity for the patient.
Sentinel node biopsy is one of the most meaningful advances in breast cancer surgery over the past two decades, and for more on what breast surgery involves overall, our blog on latissimus dorsi covers reconstruction options in detail.
Why Choose Dr. Sandeep Nayak for Breast Cancer Treatment ?
Dr. Sandeep Nayak brings 24 years of surgical oncology experience, DNB qualifications in Surgical Oncology and General Surgery and a fellowship in Laparoscopic and Robotic Onco-Surgery to every breast cancer operation including sentinel node procedures. He heads Oncology Services across Karnataka and leads breast cancer surgery at KIMS Hospital, Bangalore, with originator credits for RABIT and over 25 published clinical studies. Patients wanting clarity on nodal assessment, staging or their full surgical plan are seen here with every decision going through tumour board review. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
Is sentinel lymph node biopsy a separate operation?
No, it’s performed during the same breast cancer surgery under the same anaesthetic with no separate recovery.
What happens if the sentinel node contains cancer cells?
The team decides between full axillary dissection or axillary radiation depending on extent of involvement and treatment plan.
Does a clear sentinel node mean cancer hasn't spread anywhere?
It means the axillary nodes are almost certainly clear distant spread is assessed separately through staging scans.
How accurate is sentinel lymph node biopsy in finding cancer?
Experienced surgeons correctly identify nodal status in over 95% of sentinel node procedures performed.
References
-
- National Cancer Institute — Sentinel Lymph Node Biopsy
- National Institutes of Health — Breast Cancer Nodal Staging
- Disclaimer: The information shared in this content is for educational purposes and not for promotional use.