When Is Pain in Cancer a Surgical Emergency?
Most cancer pain is chronic and managed with medication. But some pain in cancer patients signals something acute and structural. Obstruction, perforation, bleeding, spinal cord compression. These aren’t pain management problems. They’re surgical problems. And the window between symptom onset and irreversible damage can be hours, not days.
According to Prof. Dr. Sandeep Nayak, Surgical Oncologist in India, “Cancer patients and families sometimes wait too long with sudden severe pain because they assume it’s part of the disease. Sometimes it is. But sometimes it’s a perforation or a cord compression that needs an operating theatre or emergency imaging within hours. The rule I give families is simple. If the pain is sudden, severe and different from what’s been there before, go to a surgeon the same day. Don’t manage it at home.”
Sudden severe pain in a cancer patient is not routine. It needs same-day assessment.
What Types of Pain Signal a Surgical Emergency?
Four situations change cancer pain from chronic to urgent.
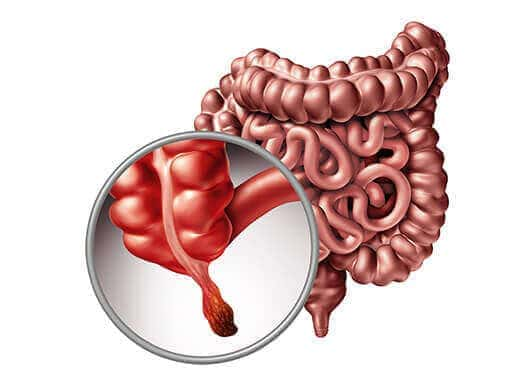
- Bowel obstruction: Crampy, colicky, worsening abdominal pain with bloating, no bowel movements and vomiting. Colon, ovarian and peritoneal cancers are common causes. If the bowel perforates, it becomes a life-threatening emergency within hours. Go to hospital, not a GP.
- Perforation: Sudden onset, severe abdominal pain, rigid abdomen, fever. A tumour has eroded through the bowel wall or stomach. Air under the diaphragm on X-ray confirms it. Needs emergency surgery. Minutes matter here.
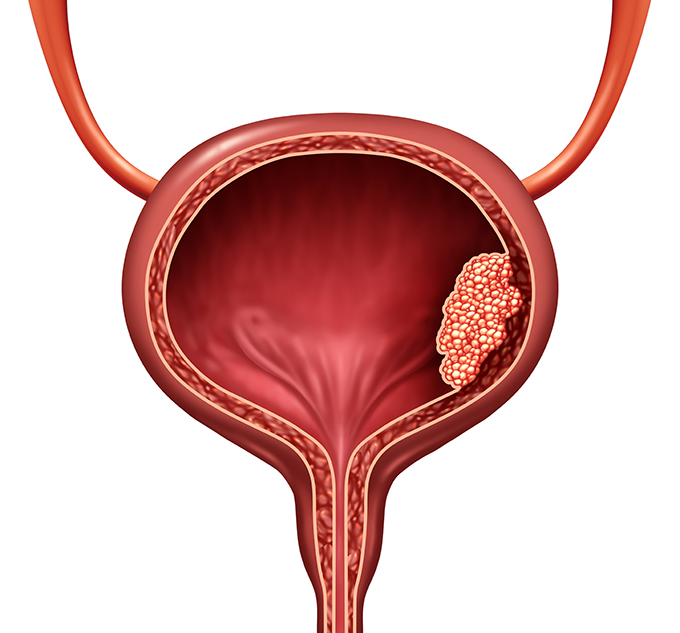
- Haemorrhage: Sudden severe pain in the abdomen or flank alongside dropping blood pressure, rapid pulse or visible blood in stool or urine. Tumour bleeding can be catastrophic. Stable patients may be embolised. Unstable ones need the operating theatre.
- Spinal cord compression: Sudden severe back pain with progressive leg weakness, numbness or loss of bladder or bowel control. Bone metastases compressing the spinal cord. Same-day MRI and often emergency surgery or radiation within 24 hours. Every hour of delay reduces the chance of neurological recovery.
For cancer patients who reach emergency surgery, robotic cancer surgery is available for appropriate elective cases but true surgical emergencies are managed with whatever approach gets the patient safe fastest.
What Distinguishes Surgical Emergency Pain From Chronic Cancer Pain?
The distinction is in the character of the pain, not just the intensity.
- Sudden onset vs gradual: Chronic cancer pain builds over days or weeks. Surgical emergency pain often strikes sharply within minutes. A patient who was comfortable two hours ago and is now writhing needs urgent assessment, not a dose increase.
- New location or new character: Pain in a familiar site that suddenly shifts character, from dull ache to sharp cramp or constant burning, suggests something structural has changed. Obstruction, bleeding and perforation all change the pain character before the clinical signs appear.
- Associated features: Fever with abdominal pain. Leg weakness with back pain. Absence of bowel sounds with distension. These combinations move the assessment from pain management into emergency surgery territory immediately.
- Failure to respond to opioids: Visceral pain from obstruction or perforation often doesn’t respond to typical opioid doses the way chronic cancer pain does. A patient taking regular morphine who reports no relief from additional doses has a warning sign that something acute is happening.
For patients and families wanting to understand how cancer surgery decisions are made generally, our blog on cancer surgery explains the full clinical picture including when urgency applies.
Why Choose Dr. Sandeep Nayak for Cancer Surgical Emergencies?
Dr. Sandeep Nayak has spent 24 years in surgical oncology. He holds DNB qualifications in Surgical Oncology and General Surgery, plus a fellowship in Laparoscopic and Robotic Onco Surgery. He manages surgical emergencies in cancer patients including bowel obstruction, perforation, haemorrhage and post-operative complications, working with the emergency and ICU teams at KIMS Hospital to stabilise and operate when the clinical picture demands it.
What makes surgical emergencies in cancer patients different from standard emergencies is the background disease. Getting it right requires a surgeon who understands both the oncological context and the acute presentation, not just one or the other. Call +91 8104310753 to book your consultation.
Frequently Asked Questions
When is cancer pain a surgical emergency?
When it signals obstruction, perforation, bleeding or spinal cord compression.
What does bowel obstruction pain feel like in cancer?
Crampy, colicky, worsening pain with bloating and no bowel movements.
Is back pain in cancer ever an emergency?
Yes, sudden severe back pain with leg weakness needs same day imaging.
Should cancer patients go to emergency for sudden severe pain?
Yes, sudden severe pain in a cancer patient always warrants urgent assessment.
Disclaimer: This blog is for informational purposes only and is not a substitute for professional medical advice.