Robotic cancer surgery takes anywhere from two hours to eight or more depending on which cancer you’re having removed, how complex your anatomy is, whether lymph node dissection is part of what needs doing and whether previous surgery has left adhesions that need working through before anyone gets near the tumour, so anyone quoting you a single number without knowing your specific case is giving you an average that may have very little to do with how long you’ll actually be on the table.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Operating time in robotic cancer surgery depends heavily on the specific procedure and the patient’s anatomy and quoting a single number without knowing the case doesn’t mean much.”
How Long Does Each Type of Robotic Cancer Surgery Take?
These are the approximate operating times for the most common robotic cancer procedures:
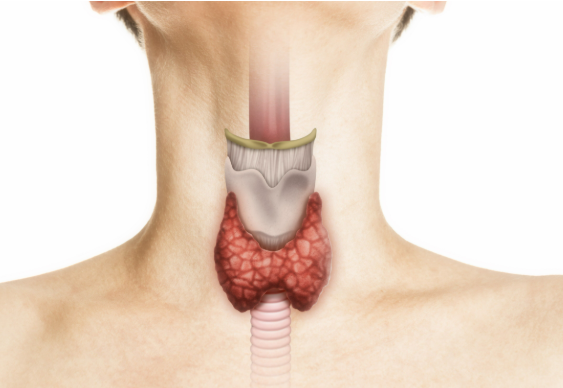
Thyroid cancer: RABIT and similar robotic thyroid approaches take two to four hours because the instruments travel through a tunnel from the armpit to the neck rather than going straight in, which adds setup and dissection time conventional open thyroid surgery simply doesn’t have.
Rectal cancer: Robotic low anterior resection and inter-sphincteric resection typically run three to five hours because the narrow pelvis, the sphincter preservation work and the precise dissection around nerves all take time that open surgery in a wider field doesn’t need to account for the same way.
Prostate cancer: Robotic prostatectomy runs two to four hours at experienced centres and the extra time compared to some open approaches goes into the nerve sparing work that makes the functional difference patients actually care about after surgery.
Colorectal cancer: Robotic hemicolectomy with D3 lymph node dissection takes two to four hours depending on tumour location, patient build and whether the vessel work during mesocolic dissection is straightforward or more involved than imaging suggested it would be.
High volume centres doing robotic cancer surgery regularly tend to run shorter operating times than lower volume centres and that’s not because they cut corners, it’s because familiarity with setup, anatomy and procedure steps means less time figuring things out mid-operation.Robotic cancer surgery at a specialist centre with a dedicated robotic team means the efficiency built from doing this repeatedly rather than occasionally is something you actually benefit from on the table.
What Factors Make Robotic Cancer Surgery Take Longer?
These are the things that push your operating time beyond the typical range for any robotic procedure:
Old scars inside: Adhesions from previous abdominal or pelvic surgery turn what should be clear tissue planes into a slow careful dissection and what normally takes an hour can easily take two if the adhesions are dense enough that rushing them creates a bleeding risk.
Tumour position: A tumour sitting right against a major vessel or in a location that limits how the instruments can approach it takes longer to remove safely regardless of how experienced the surgeon is because the physics of the situation don’t change with experience.
Lymph node work: Extended lymphadenectomy like D3 resection or central neck dissection adds real time to any robotic procedure because clearing node basins at vessel origins is systematic careful work that can’t be done faster without making it less thorough.
Your build and anatomy: Obesity, a narrow pelvis, a short thick neck or other anatomical factors that reduce the working space for robotic instruments consistently push operating time up because the surgeon is working in a smaller environment than the time estimates assume.
What your specific procedure is likely to take is something your surgical team can estimate much more accurately once they’ve looked at your imaging and understood your anatomy rather than giving you a generic number from a website.Laparoscopic cancer surgery at specialist centres covers the full minimally invasive range where operating time and case complexity get individually assessed before anything gets booked.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Dr. Sandeep Nayak has been doing robotic cancer surgery for over 15 years and the efficiency of his team at MACS Clinic in Bangalore comes from doing this at real volume rather than occasionally, which matters because time under anaesthesia is itself a risk factor especially for older patients or those carrying other health conditions going into surgery. He chairs Oncology Services across Karnataka. Dr. Nayak will tell you realistically how long your procedure is likely to run, what drives that estimate for your specific case and what it means for your recovery rather than quoting a reassuring number that has nothing to do with what’s actually on your scan.
Frequently Asked Questions
How long does robotic cancer surgery take? Two to eight hours typically depending on cancer type, procedure complexity, lymph node dissection and patient anatomy.
Why does robotic surgery sometimes take longer than open surgery? Setup time, tunnel approaches for certain procedures and the precision dissection that makes robotic surgery worth doing all add time open incisions don’t require.
Does previous surgery affect how long robotic cancer surgery takes? Yes, internal adhesions from prior operations slow dissection significantly and can add one to two hours beyond the typical range for the procedure.
Does time on the table affect recovery after robotic cancer surgery? Yes, longer anaesthesia and operating time increases risk and recovery complexity particularly for older patients or those with existing health conditions going in.
Scarless thyroid surgery in India using RABIT typically costs between one lakh fifty thousand and three lakh rupees depending on the centre, the surgeon’s experience, the hospital facility charges and whether the procedure is for thyroid cancer or a benign condition, and while that range is higher than conventional open thyroidectomy the comparison isn’t just about the operation itself because what you’re also comparing is a visible neck scar you carry for life against incisions that disappear completely under normal clothing and most patients who’ve thought that through carefully don’t find the cost difference as difficult to justify as they expected.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “The cost of scarless thyroid surgery reflects the robotic technology, the surgical expertise and the longer operating time involved and patients deserve to understand exactly what they’re paying for before they decide.”
What Affects the Cost of Scarless Thyroid Surgery in India?
These are the key factors that determine where your RABIT procedure sits within the cost range:
Robotic system usage: RABIT uses a surgical robot and the per-procedure cost of operating that system is a real component of what you pay, separate from the surgeon’s fee and hospital charges, and centres doing higher robotic volumes spread that cost more efficiently than low volume centres charging the same rate.
Surgeon experience: A surgeon who has performed hundreds of RABIT procedures charges differently from one who has done dozens and that fee difference is directly connected to the depth of experience that reduces your complication risk and operating time rather than being arbitrary.
Hospital facility: RABIT performed at a dedicated surgical oncology centre like MACS Clinic with a team built around doing this regularly carries different facility costs from a large corporate hospital adding robotic thyroid surgery to a long menu of procedures it offers at general scale.
Cancer vs benign: Thyroid cancer cases requiring neck dissection alongside RABIT are more complex procedures than straightforward benign thyroid disease removal and that added complexity affects operating time, team requirements and the overall procedure cost in ways that get reflected in the final number.
The cost of RABIT in India is significantly lower than the same procedure in South Korea, Japan or the United States where the technique originated as a category and most international patients comparing options find that the combination of Dr. Nayak’s specific experience as the RABIT developer and the Indian cost structure makes MACS Clinic the most compelling option available to them globally.Thyroid cancer treatment at MACS Clinic covers the full cost discussion transparently before any decision gets made.
Is Scarless Thyroid Surgery Worth the Cost Compared to Conventional Surgery?
These are the things patients consistently weigh when comparing RABIT cost against conventional open thyroidectomy:
Scar for life: Conventional thyroidectomy leaves a horizontal scar across the front of the neck that is visible every day for the rest of your life and for younger patients, professionals and anyone who thinks carefully about what that means over decades the cost difference often looks different than it did before they thought it through.
Recovery difference: RABIT patients generally go home within two to three days and return to normal activity faster than conventional open thyroid surgery and when you factor in the economic cost of additional recovery time away from work the gap between RABIT and conventional surgery narrows from the patient’s perspective.
Same cancer outcomes: RABIT delivers equivalent cancer control to open thyroidectomy for appropriate cases and paying more for the scarless approach doesn’t mean accepting a compromise in oncological outcome which is the most important reassurance patients need before cost becomes a meaningful factor.
Psychological value: Living without a visible scar from a cancer diagnosis is something patients value differently and some people find the psychological weight of that scar heavier than others but for those who feel it strongly the cost of avoiding it is straightforwardly worth paying.
Whether RABIT is worth the cost difference for your specific situation depends on your values, your circumstances and an honest conversation about whether you qualify for the procedure before the financial comparison becomes relevant.Robotic cancer surgery at MACS Clinic covers the full robotic oncology spectrum where cost transparency is part of how Dr. Nayak’s team approaches every patient consultation.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Dr. Sandeep Nayak developed RABIT and has been performing it longer than anyone else in India which means the experience component of what you’re paying for at MACS Clinic is genuine rather than aspirational. He chairs Oncology Services across Karnataka and sees patients at MACS Clinic in Bangalore where the cost discussion happens before treatment decisions get made rather than after. Dr. Nayak will tell you honestly whether RABIT is appropriate for your case, what it will cost specifically for your procedure and whether the investment makes sense for your situation rather than assuming every patient with the budget should have the scarless option.
Frequently Asked Questions
What is the cost of scarless thyroid surgery in India? RABIT scarless thyroid surgery in India typically costs between one lakh fifty thousand and three lakh rupees depending on the centre, surgeon experience, facility and procedure complexity.
Why does scarless thyroid surgery cost more than conventional thyroidectomy in India? Robotic system usage, longer operating time, specialist surgical expertise and dedicated facility requirements all contribute to the higher cost compared to conventional open thyroid surgery.
Is scarless thyroid surgery covered by insurance in India? Coverage varies by insurer and policy and patients should confirm with their specific provider whether robotic thyroid surgery is included before planning the procedure financially.
Is RABIT scarless thyroid surgery cheaper in India than abroad? Yes, significantly, RABIT in India at specialist centres costs a fraction of what the same procedure costs in South Korea, Japan or the United States making India the most cost-effective option for international patients.
Robotic thyroidectomy without a neck scar in India is performed by Prof. Dr. Sandeep Nayak at MACS Clinic in Bangalore using RABIT, a technique he developed himself that takes the thyroid out through incisions in the armpits and just below the collarbones so the neck stays completely untouched, and the reason this matters to patients isn’t vanity it’s that a visible scar running across the front of the neck is something you look at every day for the rest of your life and for most people who’ve just been through a thyroid cancer diagnosis that’s a burden they’d rather not carry if there’s a surgical option that removes it.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “RABIT was developed because patients deserved a way to have their thyroid removed completely without spending the rest of their life explaining a scar on their neck to everyone who notices it.”
Who Performs Robotic Thyroidectomy Without a Neck Scar in India?
These are the key things to understand about who actually does this procedure in India and what separates serious practitioners from centres that have the equipment but not the volume:
Dr. Sandeep Nayak: The developer of RABIT himself, over 24 years in surgical oncology, over 15 years doing robotic thyroid surgery in India at a time when almost no one else in the country was attempting it, sees patients at MACS Clinic in Jayanagar Bangalore from Monday to Saturday 3pm to 6:30pm.
Volume matters here: RABIT requires creating a surgical tunnel from the armpit and infraclavicular incisions to the thyroid in the neck and navigating that space with robotic instruments takes familiarity you only build through hundreds of cases not by offering the procedure because the equipment is available.
RABIT vs imported techniques: Some centres offer robotic thyroidectomy through Korean or American techniques developed elsewhere and while these work for selected patients RABIT was built specifically for the Indian patient population and anatomical variations that Dr. Nayak encountered operating here rather than adapting a foreign protocol.
Not every patient qualifies: Body proportions that make the tunnel distance unmanageable, thyroid cancer that’s spread extensively beyond the gland or surgical fitness that doesn’t support a longer operation are all reasons RABIT may not be appropriate and a surgeon who tells every patient they qualify is not being straight with them.
The honest reality is that scarless robotic thyroidectomy in India is available at very few centres with the case volume and the specific technique to do it safely and the patients who benefit most are the ones who find those centres before they agree to conventional thyroid surgery somewhere else.Thyroid cancer treatment at MACS Clinic starts with an honest assessment of whether RABIT is appropriate for your specific thyroid case rather than a blanket offer of the technique to everyone who asks for it.
What Should You Know Before Choosing Robotic Thyroidectomy Without a Neck Scar?
These are the things patients need to understand before committing to scarless robotic thyroid surgery in India:
Cancer control first: RABIT delivers equivalent cancer control to conventional open thyroidectomy for the right cases and that equivalence is the most important thing to confirm before any conversation about scars because removing the cancer completely is what everything else depends on.
Longer operating time: RABIT takes two to four hours compared to around one hour for conventional thyroid surgery and your general fitness and anaesthesia risk need to comfortably support the longer procedure before it becomes the right choice for your situation.
Hidden incisions not invisible: The scars from RABIT sit in the armpit and just below the collarbone where clothing covers them completely and they’re not visible in normal daily life but they exist and patients deserve to know that rather than imagining the procedure leaves no marks anywhere.
Follow-up is the same: Post-operative radioiodine, thyroid hormone replacement and TSH suppression after RABIT are identical to what follows conventional thyroidectomy because the surgical approach changes how you get to the gland not what happens to the cancer after it’s out.
Whether RABIT is the right surgical approach for your thyroid cancer needs your ultrasound, your cytology, your staging and an honest conversation with a surgeon who has done enough of them to know exactly where the technique works well and where it doesn’t.HIPEC treatment at MACS Clinic represents the same level of surgical specialisation across all the cancer types Dr. Nayak treats where the approach is always built around what your specific case actually needs.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
RABIT exists because Dr. Sandeep Nayak spent years watching thyroid cancer patients come through surgery cured of their disease and go home carrying a neck scar they hadn’t asked for and didn’t need to have when the surgical pathway to avoid it was something he could build if he worked it out properly. He did. He chairs Oncology Services across Karnataka and sees patients at MACS Clinic in Bangalore where Dr. Nayak will look at your thyroid case specifically and tell you whether RABIT is the right approach for your tumour, your anatomy and your fitness rather than offering it to every patient with a thyroid diagnosis because it sounds like the better option.
Frequently Asked Questions
Which doctor does robotic thyroidectomy without neck scar in India?
Prof. Dr. Sandeep Nayak at MACS Clinic in Bangalore developed and performs RABIT, a robotic thyroidectomy technique with no incision on the neck, contact plus 91 9482202240.
What is RABIT thyroid surgery?
Robotic Axillo-Bilateral Infra-clavicular Thyroidectomy, a scarless thyroid removal technique developed by Dr. Sandeep Nayak where incisions go into the armpits and below the collarbones rather than the neck.
Is scarless robotic thyroidectomy safe in India?
Yes for the right patients, RABIT delivers equivalent cancer control to conventional thyroidectomy with no visible neck scar as the outcome at high volume specialist centres.
Who is suitable for robotic thyroidectomy without a neck scar?
Patients with thyroid cancer or benign thyroid disease where the cancer hasn’t spread extensively, body proportions that allow the tunnel approach and fitness for a longer operating time.
Robotic cancer surgery is better than open surgery in India for specific cancer types in specific anatomical locations operated on by surgeons doing it at real volume but that answer falls apart the moment you apply it as a blanket statement because a tumour that’s locally advanced, a pelvis full of adhesions from prior surgery or a robotic programme that does fifteen cases a year are situations where open surgery by an experienced team is honestly the better option and any surgeon who tells you robotic is always better is selling you something.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Robotic surgery isn’t better than open surgery in every situation but in the right anatomical locations and with the right surgeon it delivers outcomes open surgery in those spaces genuinely cannot match.”
Where Is Robotic Cancer Surgery Better Than Open Surgery?
These are the situations where robotic surgery consistently delivers better outcomes than open for cancer:
Tight pelvis: Rectal cancer, prostate cancer and gynaecological cancers operated on deep in the pelvis are where robotic surgery changes what’s achievable because the magnified view and wristed instruments work in angles and planes hands in a tight enclosed space physically can’t replicate cleanly.
Nerve sparing: Operations where preserving nerves controlling bladder and sexual function is the difference between a good outcome and a serious lasting complication show measurably better preservation rates with robotic surgery than open in the same anatomical territory.
No external scar: RABIT removes the thyroid with no cut on the neck and TORS removes base of tongue tumours through the mouth rather than through the jaw and for patients who’d otherwise carry a visible scar for decades that’s not a cosmetic preference it’s something they live with every morning.
Recovery gap: Less blood loss, home in days not weeks, back to normal life significantly earlier, for someone already carrying a cancer diagnosis the difference in what treatment physically costs them is not a minor point it’s a substantial part of what they actually go through.
The outcomes data at high volume robotic cancer surgery centres in India has been building long enough now that this isn’t a novelty technology argument anymore and the patients who benefit most consistently know it from their own recovery without needing to read a paper about it.Robotic cancer surgery at a specialist surgical oncology centre in Bangalore is a standard of care conversation for the cancer types where the evidence is clear rather than a premium option the patient has to fight for.
Where Does Open Surgery Still Make More Sense?
These are the situations where open surgery is genuinely the right call even at a centre with full robotic capability:
Locally advanced tumours: Cancer that’s grown into surrounding structures, encasing major vessels or requiring complex reconstruction beyond what robotic instruments can manage reliably needs the access and tactile feedback that open surgery gives a surgeon in a way the robotic console doesn’t.
Heavy adhesions: Multiple previous abdominal operations leave scar tissue that makes robotic port placement risky and working space inadequate and the right call in that situation is open surgery from the start not a conversion mid-procedure after the port sites are already made.
Low volume robotic centres: An experienced open surgeon at a specialist centre is a better option than a robotic programme that does this procedure occasionally and any patient comparing their options should be asking specifically how many of their procedure the surgeon does robotically per year not just whether the hospital has the machine.
Emergencies: Emergency cancer surgery, cases needing immediate bleeding control and operations where unexpected intraoperative findings demand fast adaptation all favour open surgery because the setup time and instrument constraints of the robotic system become problems rather than advantages in those situations.
Whether robotic or open surgery fits your specific cancer, your anatomy and your prior treatment history is a question that needs your imaging and a surgeon who does both at enough volume to give you an honest answer about which one actually gives your case the best result.Laparoscopic cancer surgery covers the full minimally invasive spectrum at specialist centres in India where the surgical approach gets matched to the case rather than the available equipment.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Dr. Sandeep Nayak has been doing robotic cancer surgery for over 15 years and open cancer surgery for over 24 and the reason patients trust his view on which approach fits their case is that he has no reason to push one over the other because he does both at real volume and the only variable he’s optimising for is what gives your specific cancer the best outcome. He chairs Oncology Services across Karnataka and sees patients at MACS Clinic in Bangalore. Dr. Nayak will look at your tumour, your staging and your anatomy and tell you straight whether robotic surgery gives your case something open surgery genuinely can’t or whether open surgery is honestly the better fit for what’s in front of him.
Frequently Asked Questions
Is robotic cancer surgery better than open surgery in India?
For the right cancer types in anatomically difficult spaces yes, but not universally and the answer depends on your specific tumour, stage and the surgeon’s volume with your procedure.
Which cancers benefit most from robotic over open surgery in India?
Rectal, prostate, thyroid and gynaecological cancers in narrow or complex anatomical spaces show the most consistent benefit from robotic approaches over open surgery.
Does robotic cancer surgery cost more than open surgery in India?
Yes but for the right cases faster recovery, shorter hospital stay and lower complication rates offset a meaningful part of the cost difference over the full treatment period.
Can all cancer surgeons in India do robotic surgery?
No, it requires specific training, the right equipment and real case volume and outcomes at low volume robotic centres are not the same as at high volume specialist ones.
Dr. Sandeep Nayak is different from most oncologists in India because he didn’t build his reputation by treating cancer the way everyone else was treating it, he built it by developing surgical techniques that didn’t exist before he made them, operating robotically and laparoscopically on cancers that most centres were still doing open a decade after minimally invasive technology was available and consistently telling patients what was genuinely achievable for their specific case rather than what was easiest to offer.
According to Prof. Dr. Sandeep Nayak,Surgical Oncologist in India, “Every cancer patient deserves a surgical plan built around their specific tumour, their anatomy and their life rather than a protocol that was designed for the average case and applied to everyone.”
What Sets Dr. Sandeep Nayak Apart Technically?
These are the things that distinguish Dr. Nayak’s surgical practice from most oncologists in India:
Original techniques: RABIT, MIND and RIA-MIND are surgical techniques Dr. Nayak developed himself and they exist because he identified gaps in what conventional surgery was offering patients and built the technical solutions to close them rather than waiting for someone else to do it.
Robotic surgery early: Dr. Nayak got into robotic and laparoscopic cancer surgery over 15 years ago when most Indian oncology centres hadn’t committed to it and that head start built a depth of experience with robotic dissection in difficult anatomical spaces that centres adopting it later are still catching up to.
Scarless thyroid surgery: RABIT removes the thyroid through armpit and infraclavicular incisions with no cut on the neck and for a patient who would otherwise carry a visible neck scar for decades that difference is not cosmetic it’s something they live with every single day.
Sphincter preservation: Operating deep in the narrow pelvis with the precision that inter-sphincteric rectal resection demands, Dr. Nayak gives patients with low rectal cancer a realistic chance at avoiding permanent stoma in cases where open surgery or a less experienced surgeon would make a bag the default outcome.
The technical depth Dr. Nayak has built across specific cancer types at real volume over 24 years is what separates his practice from an oncologist who operates broadly across many cancer types without the same depth in any of them.Robotic cancer surgery at MACS Clinic represents the full range of minimally invasive capability that serious surgical oncology in India should be offering every patient whose tumour allows it.
What Sets Dr. Sandeep Nayak Apart as a Clinician?
These are the things patients consistently say set their experience with Dr. Nayak apart from other oncologists they consulted:
Honest assessment: Dr. Nayak tells patients what the surgical options genuinely are for their specific tumour rather than what sounds most reassuring or what’s easiest to offer and patients who’ve had consultations elsewhere notice that difference immediately.
Case specificity: Every patient gets a surgical plan built around their actual imaging, their pathology, their anatomy and their life circumstances rather than a standard protocol adjusted slightly for each new case that comes through the door.
No unnecessary surgery: Dr. Nayak is as clear about what doesn’t need operating on as he is about what does and patients who come in expecting to be pushed toward surgery often leave with a surveillance plan or a non-surgical recommendation that other centres hadn’t offered them.
Patient outcomes first: The decisions at MACS Clinic are driven by what the evidence says gives the patient the best oncological outcome and functional result not by what’s technically impressive or what fits the centre’s capabilities most conveniently.
What patients remember most after seeing Dr. Nayak isn’t just the surgery, it’s that they understood what was happening to them, why the plan was what it was and what the realistic outcomes looked like before they agreed to anything.Laparoscopic cancer surgery at MACS Clinic covers the full minimally invasive spectrum where every surgical decision starts with what your specific cancer actually needs rather than what the centre does most.
Why Choose Dr. Sandeep Nayak for Cancer Treatment?
Over 24 years in surgical oncology. Chairman of Oncology Services across Karnataka. Developer of RABIT, MIND and RIA-MIND. 15 plus years doing robotic and laparoscopic cancer surgery before most Indian centres made the decision to invest in it. Alumni of Kidwai Memorial Institute of Oncology Bangalore. These aren’t credentials assembled for a website, they’re the output of a surgeon who kept operating at the frontier of what minimally invasive oncology could offer patients rather than settling at the level most centres in India were comfortable with. Dr. Nayak sees patients at MACS Clinic in Bangalore where the standard of care is built around what the best evidence says patients deserve rather than what’s easiest to deliver at scale.
Frequently Asked Questions
What makes Dr. Sandeep Nayak different from other oncologists?
He developed original surgical techniques including RABIT, MIND and RIA-MIND, adopted robotic cancer surgery 15 years ago and consistently offers patients case-specific surgical plans rather than standard protocols.
What techniques did Dr. Sandeep Nayak develop?
RABIT for scarless thyroid surgery, MIND and RIA-MIND for precise pelvic and colorectal cancer surgery, techniques he built to address gaps conventional surgery wasn’t closing for patients.
How long has Dr. Sandeep Nayak been doing robotic cancer surgery?
Over 15 years, making him one of the earliest adopters of robotic surgical oncology in India at a time when most centres hadn’t yet committed to the technology.
Where does Dr. Sandeep Nayak see patients?
At MACS Clinic in Jayanagar, Bangalore, Monday to Saturday from 3pm to 6:30pm, contact number plus 91 9482202240.
Dr. Sandeep Nayak, a board-certified surgical oncologist (M.ch ., D.N.B.), specializes in minimally invasive cancer surgery, including robotic and laparoscopic techniques.